
19 Dec 2025
As amyloid immunotherapy enters clinical care in more countries, providers the world over are eager for more information on how well it works, and especially how safe it is. To collect such data in the U.S., the first country to approve these antibodies, the Alzheimer’s Association initiated the ALZ-NET patient registry. At this year’s Clinical Trials on Alzheimer’s Disease conference, held December 1-4 in San Diego, the association’s Maria Carrillo updated attendees on the registry’s progress. Announced four years ago, ALZ-NET took some time to get up and running, but in the last year, participation has taken off. The registry now has 3,648 participants and enrolls about 50 more per week, Carrillo said.
ALZ-NET now includes 266 sites and more than 3,600 patients.
Most are white, highly educated, and in good health.
For the 600 who have been treated for a year, reported ARIA rates are low.
Co-primary investigators Gil Rabinovici of the University of California, San Francisco, and Michael Rafii of the University of Southern California, San Diego, discussed the latest ALZ-NET data on participant demographics, efficacy, and safety. Bottom line: so far, most people taking lecanemab or donanemab have remained stable, with few reported cases of ARIA. However, presenters cautioned that this is an early look at the data, and the number of people who have been treated for a year or longer remains small. Other scientists in San Diego wondered if clinicians tend to upload their best cases to the registry, skewing the results. Despite these caveats, Rabinovici called the data an encouraging beginning for clinical use of amyloid immunotherapy.
Charlie DeCarli of UC Davis likewise found the ARIA data reassuring, and expressed hope the findings would encourage more physicians to prescribe these drugs. “People need to know this is safe,” he said in San Diego.
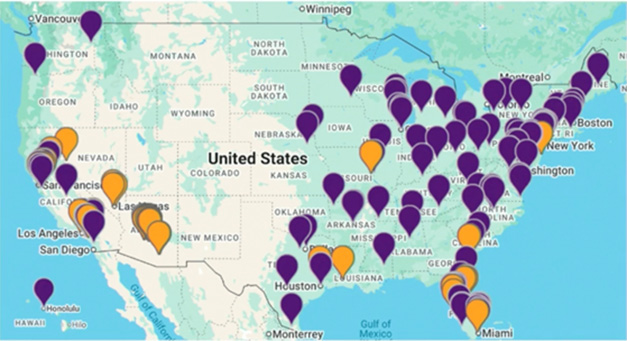
Growing Coverage. ALZ-NET currently includes 118 clinical sites (purple) and 93 imaging centers (gold) across the U.S. [Courtesy of the Alzheimer’s Association.]
Network Starts to Hum
Carrillo first announced plans for ALZ-NET at CTAD 2021, five months after aducanumab had received accelerated approval from the U.S. Food and Drug Administration (Jun 2021 news; Nov 2021 conference news). The registry is a joint undertaking: The American College of Radiology hosts the website, Brown University’s School of Public Health analyzes data, and the American Society of Neuroradiology offers additional support. ALZ-NET began enrolling patients at the end of 2022, but uptake was slow, as few people were on the new therapies and some prescribing physicians preferred the simpler CMS registry (Aug 2022 conference news; Dec 2022 conference news). Unlike the CMS registry, ALZ-NET counts as a clinical study and requires sharing data, so patients need to consent to participation.
Four years later, ALZ-NET has grown to include 118 clinical sites, with another 148 in the process of joining, Carrillo said in San Diego. Geographic distribution has broadened from the early days, with dense coverage in the eastern half of the U.S., the southwest, and California (image above). About a third of the sites are university hospitals, another third are group neurology practices, and the remainder are a mix of public and private hospitals and solo practices. In addition to clinical sites, the registry includes 93 imaging centers that help standardize data collection and serve as a repository for imaging data. Most scans are MRIs and amyloid PET, though there are some tau PET and FDG PET scans, too.
ALZ-NET is beginning to expand internationally as well. The Alzheimer’s Association has funded studies at the University of Melbourne, Australia, Amsterdam University Medical Center, and the University of Chile in Santiago to jump-start registries there, Carrillo noted.
The registry is not confined to amyloid immunotherapy patients; it will gather data on all new AD therapies approved from 2021 on. The core dataset includes a person’s medical history, diagnosis, cognitive assessments, and adverse events. Data are collected every six months for a patient’s first two years on a therapy, and annually thereafter. Registry personnel are working to automate the case reports physicians must file, in order to lighten the administrative burden, Carrillo noted.
Once uploaded, aggregate data are publicly accessible. ALZ-NET recently debuted a data dashboard that allows users to view findings and download graphics for presentations. Scientists can also submit requests for raw data, Carrillo said. Those requests go through a committee and may require an application fee.
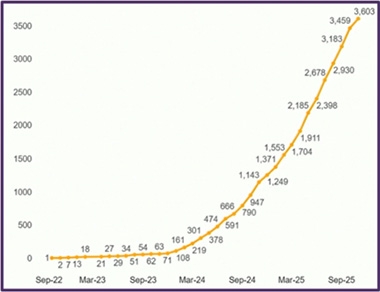
Climbing Up. ALZ-NET enrollment started rising around March 2024 and has been growing steadily since. [Courtesy of the Alzheimer’s Association.]
First Real-World Patients Look Like Trial Participants
ALZ-NET enrollment started growing in March 2024, when more people began getting lecanemab (image at right). Notably, although there are 3,648 participants as of this writing, only 1,561 have started on therapy. Of those, 80 percent are on lecanemab, 19 percent on donanemab, and 1 percent had been on aducanumab, which is now discontinued. Six people are taking the dopamine receptor agonist brexpiprazole, a new treatment for agitation (May 2023 news). So far, 50 people have withdrawn from the registry.
What do these early patients look like? Much like a typical AD trial population, Rabinovici said. Women are a majority, at 56 percent. Of the 84 percent who disclosed their race and ethnicity, 92 percent were non-Hispanic whites. Seventy percent had at least some college education. About half were taking anti-hypertensives, 40 percent were on a statin, and 14 percent were diabetic. Rabinovici noted that those chronic disease numbers are lower than would be expected for this age group, suggesting these patients are fairly healthy.
Overall, patients do not yet reflect the broader U.S. population. “We were disappointed by the lack of diversity,” Carrillo said in San Diego. “We’re working hard on improving that.”
The age range was broader than in trials, going from 47 to 97. The average is 75, again similar to trial data. Most participants had developed cognitive symptoms four years before enrolling, suggesting clinicians have work to do to catch people at earlier disease stages, Rabinovici said. The average MMSE score is 25. Overall, two-thirds of participants have mild cognitive impairment and one-third mild dementia, as expected. Intriguingly, the percentage of people with MCI has increased from 23 percent for the first-approved drug, aducanumab, to 63 percent for lecanemab, and 68 percent for the latest-approved drug, donanemab, hinting that physicians may be starting to prescribe treatment earlier.
Demographic data indicate that many clinicians are following Appropriate Use Recommendations for amyloid immunotherapies (Apr 2023 conference news; Nov 2024 conference news). Only 1 percent of ALZ-NET participants are on anti-coagulants, in keeping with the AUR advising against co-administering these drugs with amyloid immunotherapy. Eighteen percent of ALZ-NET participants take anti-platelet drugs, which the AUR do not restrict.
The AUR also recommend APOE genotyping, along with caution in prescribing to E4/4 homozygotes. Among ALZ-NET participants, 92 percent were genotyped for APOE. Two-thirds of them were APOE4 carriers, as expected for an Alzheimer’s population. Only 9 percent were homozygote, suggesting that clinicians indeed hold back on prescribing amyloid immunotherapy to them. Typically, 15 percent of AD patients are E4 homozygotes.
Rabinovici stressed that current participants represent early adopters. He expects a broader group of people will start immunotherapy over time. He noted that clinicians at UCSF are already widening their criteria for treatment, making decisions on a case-by-case basis.
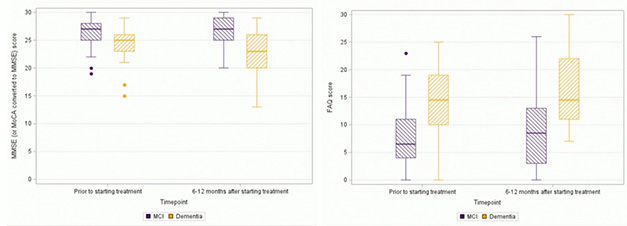
Holding Steady. On amyloid immunotherapy, MCI patients (purple) had no change on the MMSE (left) over a year, while people with mild dementia (yellow) worsened by two points. On the functional activities questionnaire (right), both groups stayed stable. [Courtesy of the Alzheimer’s Association.]
Safety Promising, But Data Skimpy
In his talk, Rafii detailed efficacy and safety data for the 607 people who started either lecanemab or donanemab after enrolling in the registry. Most have been on therapy for about a year now. MCI patients have remained stable on the MMSE during that time, Rafii said, while mild dementia patients declined two points. Both groups were unchanged on functional measures (image above). In general, people at early disease stages tend to progress slowly, with one study finding that 78 percent of people with biomarker-confirmed MCI-AD, and 64 percent with mild AD dementia, remained stable over the course of a year (Potashman et al., 2021).
ALZ-NET sites report unexpectedly low ARIA rates. In trials, ARIA-E had cropped up in 13 percent of people on lecanemab, and 16 percent of those getting donanemab on the modified titration scheme (Jul 2025 news). In ALZ-NET, by contrast, 7 percent of all participants developed ARIA-E. For APOE4 homozygotes, the rate was 15 percent (image below). Breaking the data into subgroups, ARIA-E incidence was slightly higher on donanemab than lecanemab—8.4 versus 6.1—and slightly higher for people with mild dementia than MCI, at 7.8 versus 5.6 percent. Other clinical programs have reported much higher odds of ARIA at later disease stages (May 2025 news). Meanwhile, ARIA-H rates were as expected in this registry population. In trials, the incidence of isolated ARIA-H was not altered by immunotherapy.
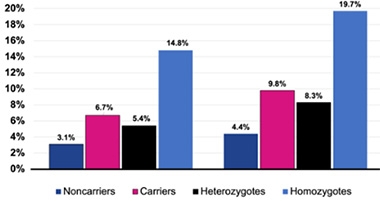
ARIA by Genotype. In the ALZ-NET dataset, APOE4 noncarriers (dark blue) have lower rates of ARIA-E (left) and ARIA-H (right) than do heterozygotes (black) and homozygotes (light blue). [Courtesy of the Alzheimer’s Association.]
To date, most ARIA documented in this registry has been mild. Rafii reported three moderate cases of ARIA-E on lecanemab, and four on donanemab. Three people on lecanemab who had recurrent episodes developed ARIA that was rated as severe on MRI scans. One person on each drug had a macrohemorrhage; no deaths were ascribed to the therapy. As for ARIA management, it varied. Slightly more than a third of participants continued dosing, a third paused until ARIA cleared up, and a quarter stopped immunotherapy.
Rabinovici cautioned that the full safety picture may be less rosy. Participant numbers remain small, especially for donanemab, where only 119 people were included in safety analyses. In addition, many people are newly on drug and may not have developed ARIA yet. “We need longer follow-up before rates stabilize,” he said in San Diego.
For his part, Rafii suggested these rates may be lower than in trials because physicians are being cautious about whom they prescribe to, for example excluding APOE4 homozygotes and people with vascular co-morbidities. Stephen Salloway of Butler Hospital in Providence, Rhode Island, warned that reporting bias could also be at play, with some cases not captured by ALZ-NET. “There have been ARIA-related deaths in clinical practice,” he reminded scientists (Aug 2024 conference news).
Other U.S. programs reported similar findings. In San Diego, neurologist Salvatore Napoli presented data on 55 AD patients treated at the Neurology Center of New England in Foxborough, Massachusetts. So far, 4 percent have developed ARIA-E, and about three-quarters have remained stable or improved on the MMSE over 18 months. This center transitioned eight patients from aducanumab to lecanemab without clinical change.
Likewise, Nicholas Frost at the University of Utah, Salt Lake City, reported little ARIA among the 70 patients taking lecanemab at his center. Three people, or 4 percent, developed ARIA-E. This cohort had been in treatment longer than most ALZ-NET participants, receiving an average of 17 doses each over two years of treatment. Another difference? Because the University of Utah serves a large geographic area, including patients from “neurologist deserts” Idaho, Montana, and Wyoming, about half the visits had to be conducted virtually. Even so, it works. “Lecanemab administration can be safely performed in distributed areas, aided by telehealth tools,” Frost concluded.—Madolyn Bowman Rogers
Therapeutics Citations
News Citations
Aducanumab Approval Sparks Backlash 22 Jun 2021
Aduhelm Lowers Tau; Registry to Track Real-World Performance 19 Nov 2021
Bringing Aduhelm—and Antibodies to Come—Into Practice 30 Aug 2022
Dare We Say Consensus Achieved: Lecanemab Slows the Disease 9 Dec 2022
FDA Approves Rexulti for Agitation in Alzheimer’s 12 May 2023
Next Goals for Immunotherapy: Make It Safer, Less of a Hassle 21 Apr 2023
Donanemab: Small Tweak in Titration, Big Gain in Safety? 8 Nov 2024
FDA Approves Safer, Slower Donanemab Titration 24 Jul 2025
In Clinical Use, Most ARIA Occurs in People With Dementia, Not MCI 16 May 2025
Two New Deaths on Leqembi Highlight Need to Better Manage ARIA 16 Aug 2024
Paper Citations
Potashman M, Buessing M, Levitchi Benea M, Cummings J, Borson S, Pemberton-Ross P, Epstein AJ.
Estimating Progression Rates Across the Spectrum of Alzheimer’s Disease for Amyloid-Positive Individuals Using National Alzheimer’s Coordinating Center Data.
Neurol Ther. 2021 Dec;10(2):941-953. Epub 2021 Aug 24
PubMed.
External Citations