
One of the loudest claims circulating on social media right now is that clinicians recommend vaccines because they profit from them.
These concerns don’t come out of nowhere. The U.S. health system is profit-driven. Insurance companies are massive corporations. Doctors, like everyone else, operate in a system shaped by money. Many Americans are in massive debt due to large medical bills. And, people are understandably fed up.
But is the claim true?
This question matters not only because the claim risks damaging the patient–physician relationship and trust, but because it’s already shaping real-world policy. On January 21, the Texas attorney general announced a formal investigation into “unlawful financial incentives” for childhood vaccines, stating he aimed to “ensure that Big Pharma and Big Insurance don’t bribe medical providers to pressure parents.” On August 8, 2025, Secretary Kennedy echoed the narrative saying, “Doctors are being paid to vaccinate, not to evaluate. They’re pressured to follow the money, not the science.”
The problem was that the data around this question (and thus the answer) was super complicated and convoluted. But a new white paper from our friends at Unbiased Science digs into the data. TL;DR: Clinicians, and specifically pediatricians, generally do not profit from vaccines.
We asked you what questions you had. And, as you’ll see below, many physician YLE readers chimed in with their context.
Usually, no. In fact, they often lose money.
Clinicians are paid for vaccines in two ways:
A small administration fee for giving the shot and counseling families, typically ranging from $7–$28, depending on insurance type and state.
Reimbursement for the vaccine itself, which is supposed to cover the cost of purchasing it. This can range from $20 to $300+. In practice, many clinics report being reimbursed at or below what they paid.
Once you factor in staff time, storage and refrigeration, insurance paperwork, and the need to purchase vaccines upfront (often months before reimbursement), most pediatric practices break even. In many practices, low reimbursement for Medicaid and uninsured vaccine administration means the practice loses money on each vaccine administered.
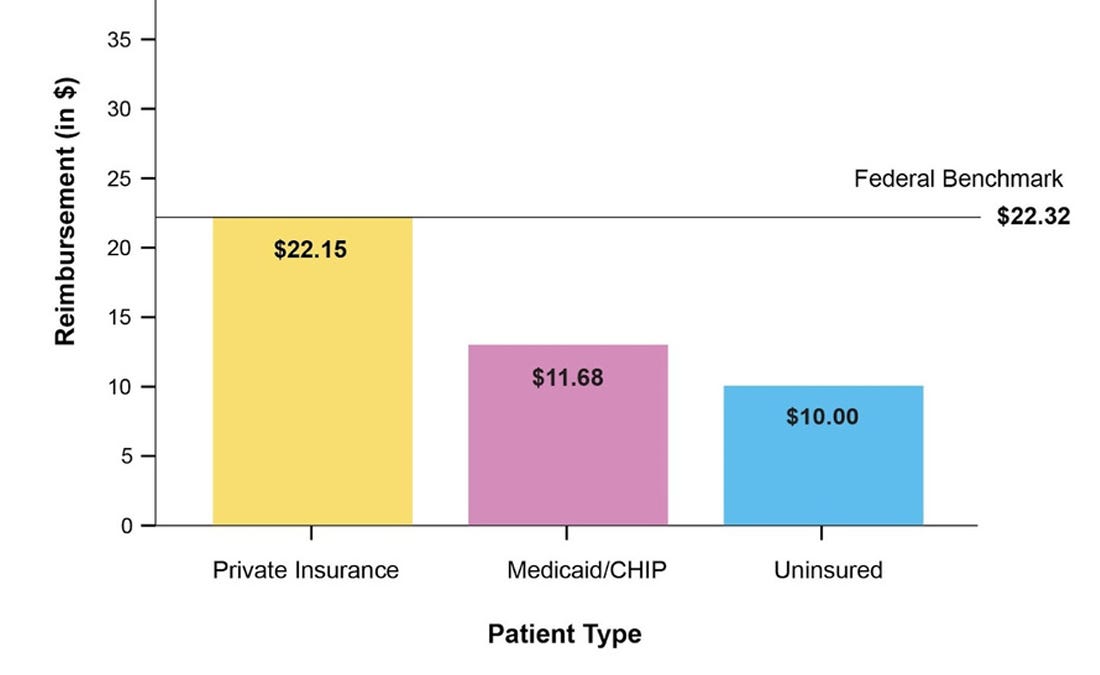
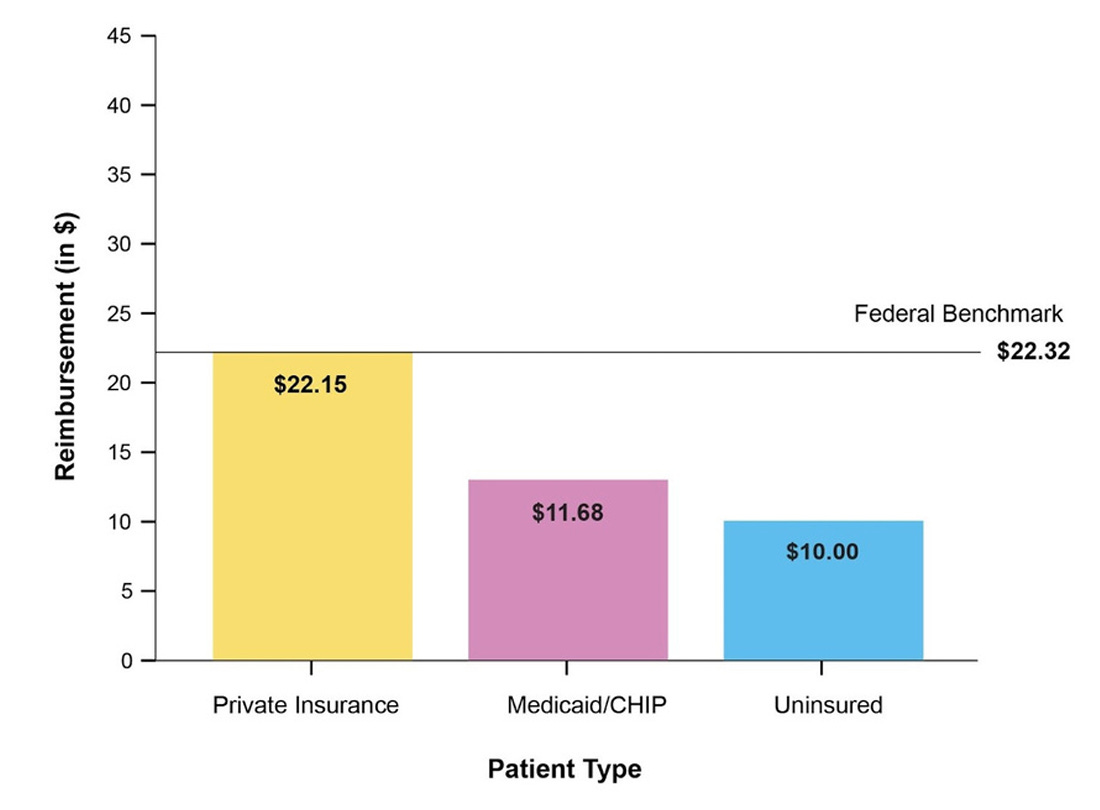
Take Mississippi, for example. They have one of the most challenging economic environments for vaccine delivery in the country. The state’s Medicaid program reimburses for vaccine administration at $11.68 per dose. This is well below a federal benchmark ($22.32) and the estimated actual cost of delivering a vaccine (~$15 or more). For patients with private insurance, providers must purchase vaccines up front, cover storage and handling costs, and then wait for reimbursement. For example, the upfront purchase price of a single DTaP dose is about $30. Taken together, this often means practices lose money, especially in states like Mississippi.
Vaccines are among the least profitable services clinicians provide. As a result, many are stepping away from vaccine delivery altogether. A national survey found:
Nearly 1 in 4 pediatricians has seriously considered stopping vaccine delivery.
The top reason was financial strain threatening their practice, not doubts about vaccine safety or science.
From the YLE Substack chat, one clinic leader who ran primary care organizations for 12 years shared a similar sentiment:
“Clinics barely break even on vaccines, and more and more primary care clinics are choosing to stop stocking vaccines and instead refer patients to health departments or pharmacies.”
Not in the way social media claims.
Some insurance companies offer quality-of-care bonuses, but these are often misunderstood. They are:
Based on many measures of good care, not vaccines alone. For example, by conducting developmental screenings, managing chronic diseases, and maintaining patient satisfaction, rather than just providing medical services and procedures.
Typically, a few hundred to a few thousand dollars total.
Not paid per shot or per child.
For example, one claim on social media that gets recycled is that pediatricians earn huge bonuses—often cited as $40,000 or more. This can be traced back to a single quality program in Michigan from years ago, but is taken out of context. If you look into the data, here’s what that program actually paid:
About $400 to $9,600 per provider.
With a maximum cap of $9,600.
Based on meeting broad quality benchmarks across dozens of areas beyond vaccines.
It’s also important to be clear: pharmaceutical companies do not pay clinicians to vaccinate children. That would violate federal anti-kickback laws, which prohibit drug manufacturers from financially incentivizing the prescribing or administration of vaccines.
Pharmaceutical companies set vaccine prices. Insurance companies decide reimbursement. Currently, insurers must cover recommended childhood vaccines with no cost-sharing, meaning most families pay nothing out of pocket for routine vaccines. That remains true this year, even amid federal changes, though what happens in 2027 is still unclear.
Payment varies by payer:
Private insurance: Covers both the vaccine and administration, usually at higher rates.
Medicaid / CHIP: Pays much less, often below the true cost of delivery.
Vaccines for Children (VFC): The government supplies vaccines free of charge, but practices receive only a small administration fee.
Families: Rarely pay out of pocket for routine childhood vaccines.
Because vaccines work and because clinicians believe preventing disease is part of their job, even when it costs their practice money.
One family doctor in Michigan described how, when families choose not to vaccinate, his quality scores drop, reducing reimbursement, even though he strongly supports vaccination and continues to accept all patients, even if they don’t want a vaccine.
A retired pediatrician in the YLE community shared the same: while vaccination rates were a quality metric in her state, she refused to drop vaccine-hesitant families just to improve scores. Maintaining trust and continuing the conversation mattered more.
If profit were the motivator, doctors would do the opposite: provide fewer vaccines, refuse federally insured patients, or focus on treating preventable diseases, which generates far more revenue than preventing them.
Clinicians, including pediatricians, aren’t vaccinating kids to make money. They’re doing it because it prevents severe disease, often while navigating a system that makes prevention financially hard to sustain. There are many reasons our health care system is utterly insane, but vaccines (an intervention that prevents severe disease and healthcare use) are not one of them.
Love, YLE
Your Local Epidemiologist (YLE) is founded and operated by Dr. Katelyn Jetelina, MPH PhD—an epidemiologist, wife, and mom of two little girls. YLE reaches more than 425,000 people in over 132 countries with one goal: “Translate” the ever-evolving public health science so that people will be well-equipped to make evidence-based decisions. This newsletter is free to everyone, thanks to the generous support of fellow YLE community members. To support the effort, subscribe or upgrade below: