

Introduction
With the widespread popularity of electronic devices, the screen time spent by people on phones, computers, and televisions has increased significantly every day. Recently, an increasing number of studies have shown that excessive screen time may bring a series of health risks [,]. A study on children and adolescents has shown that long-term screen time exposure is closely related to obesity, restricted cognitive and language development, decreased academic performance, and altered sleep patterns [,]. Studies on adults have found that excessive screen time is associated with reduced physical activity and increased BMI []. Moreover, studies have found that the incidence of headaches increases with increased screen time, with similar trends observed in both adolescents and adults [-]. Research has also shown that prolonged computer use can contribute to pain in several areas, such as the neck, shoulders, and back [].
While some studies have explored the relationship between screen time and chronic pain, the current evidence is still limited. An important limitation is that existing studies have shortcomings in assessment scope and underlying relationship to fully reveal the association between the two. We found that most studies have focused on the use of a single type of screen time. One study only pointed out that prolonged computer use can cause pain in multiple areas [], but ignored the effects of different types of screen time. Moreover, most studies on screen time and chronic pain tend to focus on specific body regions, such as lower back pain or headaches [,], while overlooking the impact of screen time on multisite chronic pain (MCP) and the combined effects of different types of chronic pain. In addition, the results of existing studies are inconsistent, with some studies finding an association between screen time and chronic pain [], while others fail to observe a significant association []. This inconsistency may be caused by confounding bias or a weaker ability to infer causality.
Another important limitation in the current research concerns the mechanisms associated with screen time and chronic pain. Some studies have suggested that the brightness or light wave frequency of screens may trigger migraine attacks, while prolonged exposure to screens may lower the threshold for migraines [-], making them more likely to be triggered by other factors. However, this explanation lacks a detailed understanding of the biological mechanisms involved. To date, the underlying biological mechanisms linking screen time and chronic pain have remained largely unexplored, highlighting the need for future research to address this issue and explore whether different devices cause chronic pain through common or different mechanisms.
The genome-wide association studies (GWASs) of MCP [], the development of genetic epidemiology, and multiomics integration analysis methods provide new opportunities to address these limitations [,]. Two-sample Mendelian randomization (MR) analysis can be used to examine the potential relationship between screen time and chronic pain. MR analysis uses genetic variants significantly associated with exposure as instrumental variables (IVs) to infer causality, thereby minimizing confusion and reverse causality []. In addition, summary data–based Mendelian randomization (SMR) and transcriptome-wide association study (TWAS) analysis can help identify overlapping genes between the two. In addition, colocalization analysis can assess whether these associations share causal genetic variation, thereby strengthening the evidence for shared biological mechanisms. By using multiple genetic epidemiological methods, we can explore the biological relationship between screen time and chronic pain.
In this study, we aimed to address these limitations. First, we examined whether screen time was associated with MCP and chronic pain in 5 other body parts. Next, we identified overlapping genes through genetic epidemiological methods approach and explored their potentially shared biological mechanism, aiming to provide new insights into the complexity of chronic pain.
MethodsStudy Overview
As shown in , this study follows a 3-stage approach. In Phase 1, we performed a 2-sample MR analysis and reverse MR to investigate the phenotypic association between screen time and chronic pain. Considering the mutual influence among multiple exposures, we conducted a multivariate Mendelian randomization (MVMR) analysis. In Phase 2, we first performed SMR analysis combined with expression Quantitative Trait Locus (eQTL) summary datasets to explore associations between gene expression and phenotypic traits. We then performed TWAS analysis to identify gene expression associated with screen time and chronic pain, and assessed whether the same genetic variants were shared through colocalization analysis, providing stronger genetic evidence. In Phase 3, we further integrated the results of SMR, TWAS, and colocalization analysis. We aimed to identify genes that were consistently supported across these methods. The overlapping genes provide more robust evidence of shared biological mechanisms in the association between screen time and chronic pain.
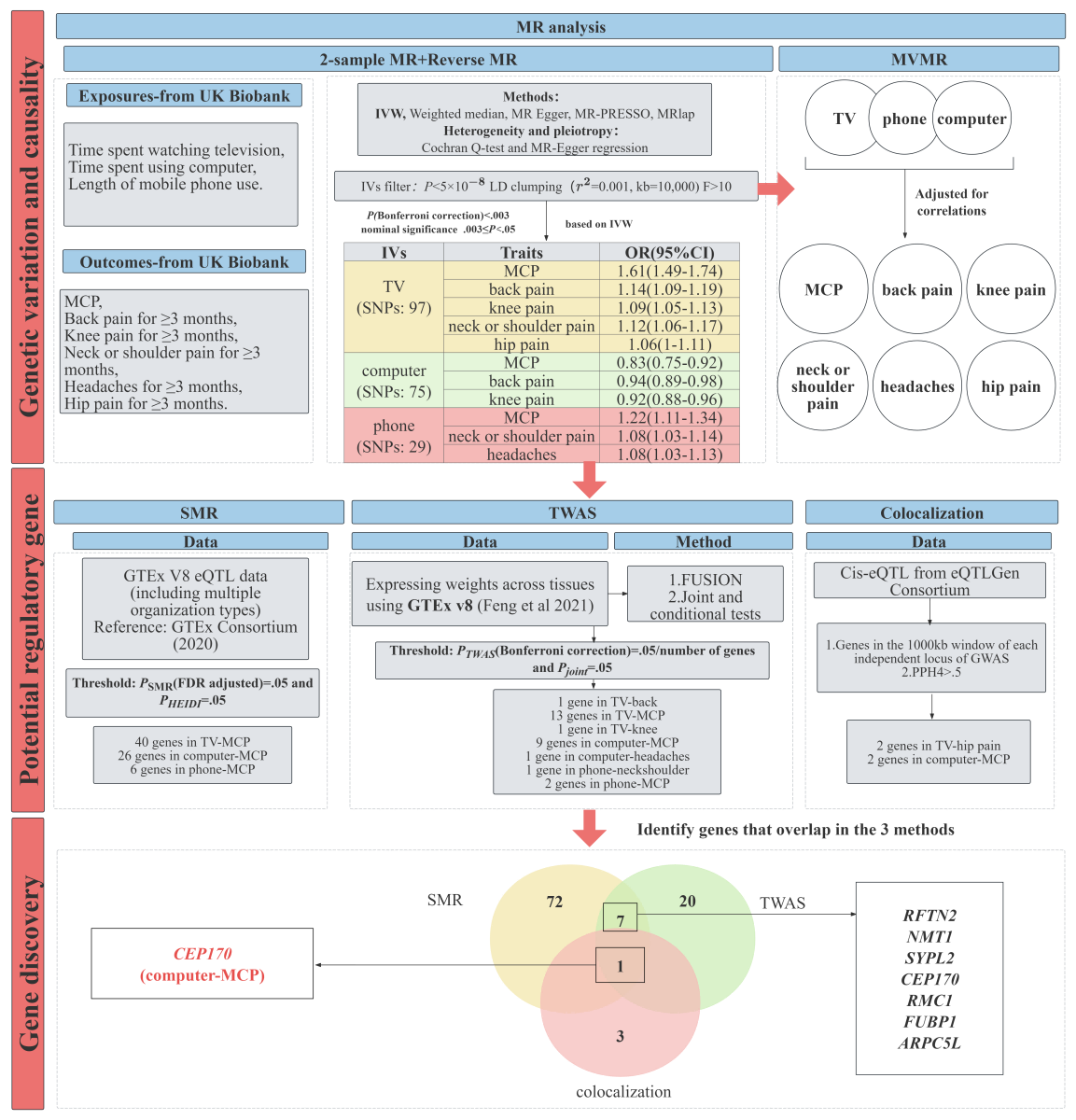 Figure 1. Flowchart of the overall study design. eQTL: expression Quantitative Trait Locus; FDR: false discovery rate; GTEx: Genotype-Tissue Expression; GWAS: genome-wide association study; IV: instrumental variable; IVW: inverse variance weighted; LD: linkage disequilibrium; MCP: multisite chronic pain; MR: Mendelian randomization; MVMR: multivariate Mendelian randomization; OR: odds ratio; SMR: summary data–based Mendelian randomization analysis; SNP: single-nucleotide polymorphism; TWAS: transcriptome-wide association study; TV: television. Data Sources for Exposures, Outcomes, and eQTL Summary DataExposures
Figure 1. Flowchart of the overall study design. eQTL: expression Quantitative Trait Locus; FDR: false discovery rate; GTEx: Genotype-Tissue Expression; GWAS: genome-wide association study; IV: instrumental variable; IVW: inverse variance weighted; LD: linkage disequilibrium; MCP: multisite chronic pain; MR: Mendelian randomization; MVMR: multivariate Mendelian randomization; OR: odds ratio; SMR: summary data–based Mendelian randomization analysis; SNP: single-nucleotide polymorphism; TWAS: transcriptome-wide association study; TV: television. Data Sources for Exposures, Outcomes, and eQTL Summary DataExposures
The exposure phenotype in this study was screen time, which included time spent watching television, time spent using computer, and length of mobile phone use. These phenotypes were derived from the UK Biobank touchscreen questionnaire. The question for time spent using computer explicitly stated, “Do not include using a computer at work,” whereas the questions for television watching and mobile phone use captured overall daily use. We provided detailed data sources about screen time in . To address the issue of weak instrument bias, a genome-wide significance threshold of P<5×10–8 was used as the default criterion for identifying single-nucleotide polymorphisms (SNPs); simultaneously, to optimize the results and eliminate SNPs in strong linkage disequilibrium (LD), an LD clustering method was adopted, with thresholds of r2=0.001 and kilobase, kb=10,000 to ensure accurate and precise clustering. r2 is the squared correlation coefficient between 2 SNPs’ allele counts, used to quantify LD. In the 2-sample MR analysis, we selected 112, 82, and 32 independently significant SNPs located on the autosomes as IVs of time spent watching television, time spent using computer, and length of mobile phone use, respectively. Details of these SNPs are presented in -.
Outcomes
The outcomes included 6 chronic pain phenotypes, namely MCP, back pain for ≥3 months, knee pain for ≥3 months, neck or shoulder pain for ≥3 months, headaches for ≥3 months, and hip pain for ≥3 months. Among them, MCP is by far the largest GWAS summary statistic for all chronic pain phenotypes, involving 387,649 people from the UK Biobank []. Data for the remaining 5 types of chronic pain came from the Integrative Epidemiology Unit (IEU) OpenGWAS, which covered a total of about 9,851,867 SNPs in both male and female individuals []. presents the sources of these outcome data. The participants were all European populations to reduce bias caused by population heterogeneity. In reverse MR analysis, shows that 31 independently significant SNPs located on the autosomes as IVs of MCP.
eQTL Data
The Genotype-Tissue Expression (GTEx) project was established to characterize the genetic influence on transcriptomic variation across human tissues and to link regulatory mechanisms to traits and diseases. GTEx v8 provides 15,201 RNA-sequencing samples from 49 tissues [], collected from 838 postmortem donors. The dataset comprehensively characterizes cis- and trans-eQTLs, revealing regulatory associations for nearly all genes and offering insights into allele heterogeneity, pleiotropy, and tissue-specific genetic effects. For SMR analysis, we used 8 eQTL summary data from GTEx (v8): Adipose Subcutaneous, Adipose Visceral Omentum, Brain Cerebellum, Brain Cortex, Brain Spinal cord cervical c-1, Muscle Skeletal, Nerve Tibial, and Whole Blood []. This is a set of cis-eQTL summary data for 8 human tissues from GTEx v8.
For colocalization analysis, we additionally used eQTL data from the eQTLGen Consortium []. eQTLGen provides a larger scale of eQTL data than GTEx, which can improve the confidence of colocalization analysis.
Statistical Analysis2-Sample MR Analysis
2-sample MR analysis was conducted for exposure and outcome. The strength of IVs was assessed using the F-statistics: F = R2× (N – 2)/(1 – R2), where R2 represents the proportion of variation in the exposure variable explained by IVs []. The calculation of R2 involved multiplying beta (the estimated genetic association of each SNP with the trait) by minor allele frequency (MAF), using the formula 2 × MAF (1 – MAF) β2. An F-statistic >10 indicates a robust instrument []. IVs with F-statistics below 10 were considered weak instruments and excluded from analysis. We applied inverse variance weighted (IVW) regression as the primary method to estimate the effects of screen time on chronic pain []. In order to assess the robustness of the results, we also performed different sensitivity analyses. First, we complement the IVW MR with the weighted median, MR-Egger methods. The weighted median method can robustly estimate the causal relationship even when less than 50% of the genetic variants are invalid IVs []. The MR-Egger method includes an intercept term to account for directional pleiotropy []. Pleiotropy means that SNPs not only affect outcomes through exposures but also directly influence outcomes through other independent pathways. However, the slope of the MR-Egger regression provides valid MR estimates in the presence of horizontal pleiotropy [,]. It should be noted that when the number of SNPs is small, the statistical ability of MR-Egger is limited, making its results less reliable []. Second, we used Mendelian Randomization Pleiotropy Residual Sum and Outlier (MR-PRESSO) to detect the presence of outliers and to reassess the effect after removing the detected outlier SNPs []. Finally, we performed a leave-one-out analysis to reevaluate the IVW effect by excluding SNPs one by one []. To investigate potential bias due to sample overlap between screen time and chronic pain, we further conducted the MRlap method []. We examined the Pdifference of MRlap results, which is the P value used to test for differences between the observed (uncorrected) and corrected effects. We used the Bonferroni correction to account for multiple tests in the IVW result. An association was considered significant if the P value in the primary analysis was below 2.778×10–3 (.05/18) and the direction of effect estimates remained consistent across all methods. Correspondingly, suggestive evidence was considered if the P value for the IVW result was between .003 and .05.
To ensure methodological rigor and robustness, we also conducted a reverse MR, which is similar to the approach of 2-sample MR.
MVMR Analysis
To clarify the independent effects of each type of screen time on chronic pain, we performed MVMR analysis. The MVMR takes into account the combined effects of multiple related exposures, thereby adjusting for potential confounders and providing a more precise estimate of the independent contribution of each exposure. In the MVMR analysis, 3 phenotypes related to screen time exposures (time spent watching television, time spent using computer, and length of mobile phone use) were used as common exposure variables, and SNPs with P<5×10–8 genomic significance were used as IVs. At the same time, SNPs in strong LD with exposure variables were removed through LD clustering (r2=0.001, kb=10,000). Next, we merged the SNPs of 3 exposures and deleted the duplicate SNPs. To ensure validity, only SNPs present in the result data were retained and any SNPs that did not match were excluded. The IVW method was used for main effect estimation. We evaluated the strength of the IVs using the conditional F-statistics, which measure the strength of each exposure conditional on the others in the model. If the conditional F-statistics for all exposures exceeded the rule-of-thumb value of 10, the IVs were considered adequately strong for the purposes of MVMR [].
SMR Analysis
We performed SMR analysis to explore whether gene expression is causally linked to both screen time and chronic pain [], thereby identifying potential functional genes involved in the relationship. SMR integrates GWAS and eQTL data, enabling the investigation of associations between gene expression and phenotypic traits. In the SMR analysis, exposures and outcomes were analyzed separately with each eQTL summary data to assess whether gene expression is linked to both screen time and chronic pain. During the analysis, SNPs significantly associated with gene expression in cis-eQTL summary data were used as IVs, as they serve as genetic proxies for gene expression levels. These SNPs were selected based on their genome-wide significant association with gene expression in eQTL summary data. False discovery rate (FDR) correction was applied to control the FDR of multiple tests. Additionally, to verify whether the observed associations could be caused by a single causal variable, we evaluated the association results using the heterogeneity in dependent instruments (HEIDI) test implemented in the SMR tool, retaining only probes with PHEIDI values indicating low heterogeneity []. Ultimately, the SMR analysis results for screen time and chronic pain were integrated to identify overlapping genes and further explore their potential roles in the association between screen time and chronic pain.
TWAS Analysis
We conducted TWAS to identify genes whose expression may mediate the relationship between screen time and chronic pain. GWAS datasets were obtained from IEU OpenGWAS, and using the FUSION tool developed by Gusev et al [], we performed single-trait TWAS using the 3 cross-tissue weights for cross-tissue features generated through sparse canonical correlation analysis (sCCA) on GTEx v8 gene expression (including sCCA1, sCCA2, and sCCA3) to identify regulatory genes that may be involved in chronic pain pathways []. To control for type I error rates, Bonferroni correction was applied to each exposure and result to interpret multiple tests, setting the significance level for each trait or tissue to P=.05/number of genes (adjusted for the number of genes on each chromosome in the 3 GTEx v8 weights). We then extracted significant GWAS of exposure and outcome, performed joint and conditional tests on loci with multiple related features to assess whether loci contain signals independent of expression. Finally, we sought overlapping genes between exposures and outcomes in joint tests.
Colocalization Analysis
To further verify the reliability of the SMR analysis results and determine whether screen time and pain are driven by the same genetic variation, we used colocalization analysis. First, we determined all independent signals of GWAS across the genome through LD independence analysis. Genes within a 1000-kb window of each independent locus were subjected to colocalization analysis []. Within these windows, we combined the corresponding genes with eQTL data, which is cis-eQTL data in SMR format, and then conducted colocalization analysis. We performed colocalization analysis using the default priors of P1=1×10–4, P2=1×10–4, and P12=1×10–5 []. Colocalization analysis assesses whether 2 traits may be driven by the same causal variant by estimating the joint posterior probability (PP) of GWAS and eQTL signals at the same locus. This method assumes a maximum of one causal variant per trait in a gene region and uses approximate Bayesian factor calculations to derive the PP for 4 mutually exclusive hypotheses (H0-H4), representing all possible association configurations between 2 traits: (1) H0: neither trait has a genetic association in the region; (2) H1 or H2: only trait 1 or trait 2 has a genetic association in the region; (3) H3: both traits are associated, but with different causal variants; and (4) H4: both traits are associated and share a single causal variant. The PP of each configuration is denoted as PPH0, PPH1, PPH2, PPH3, and PPH4, respectively []. We used PPH4 to characterize the possibility of colocalization. The probability value of .5< PPHb <.8 suggests a moderate support for colocalization, whereas PPH4≥.8 indicates a strong support for colocalization, indicating that the 2 signals share a causal variant at this locus []. Using eQTL data, colocalization analysis was conducted separately for exposure and outcome traits, and genes showing evidence of colocalization were subsequently overlapped at the gene level.
Finally, to ensure the robustness of the analysis results, we further screened and consolidated the results of 3 analysis methods. We compared the colocalized genes with the overlapping genes identified in SMR and TWAS analysis to enhance the understanding of the potential biological mechanisms of these genes in the relationship between screen time and chronic pain.
Ethical Considerations
All data used in this study were deidentified publicly available data; therefore, no ethical approval was required for this study. All original studies received ethical approval from their respective institutional review boards, and all participants provided informed consent. The data used were anonymized to ensure privacy and confidentiality. No compensation was provided to participants. Additionally, this study does not include any identifiable images or figures.
ResultsThe Putative Association Between Screen Time and Chronic Pain
The F-statistics of IVs are all greater than 10 in -, indicating that the IVs are relatively strong. We used a 2-sample MR method to make causal inference, primarily relying on the IVW method. shows that the 2-sample MR results of screen time and chronic pain based on the IVW. The box in indicates the point estimate of the causal effect, and the error bars represent the 95% CI. showed that time spent watching television and length of mobile phone use were positively associated with chronic pain, while time spent using computer was negatively associated. Our IVW results suggested significant positive associations of time spent watching television with MCP (P=1.05×10–31; odds ratio [OR] 1.61, 95% CI 1.49-1.74), back pain (P=2.41×10–8; OR 1.14, 95% CI 1.09-1.19), knee pain (P=7.10×10–6; OR 1.09, 95% CI 1.05-1.13), and neck or shoulder pain (P=1.18×10–5; OR 1.12, 95% CI 1.06-1.17). The association between time spent watching television and hip pain (P=.03; OR 1.06, 95% CI 1-1.11) reached nominal significance. It is notable that even though there is horizontal pleiotropy between time spent watching television and back pain (PMR-Egger intercept=.02), it is significant after MR-Egger correction (PMR-Egger slope=4.20×10–4). Similarly, our IVW results indicated significant positive associations of length of mobile phone use with MCP (P=2.15×10–5; OR 1.22, 95% CI 1.11-1.34), headaches (P=.003; OR 1.08, 95% CI 1.03-1.13), and neck or shoulder pain (P<.001; OR 1.08, 95% CI 1.03-1.14). However, IVW results suggested significant negative associations of time spent using computer with MCP (P<.001; OR 0.83, 95% CI 0.75-0.92), and knee pain (P=3.20×10–5; OR 0.92, 95% CI 0.88-0.96). The association between time spent using computer and back pain (P=.01; OR 0.94, 95% CI 0.89-0.98) reached nominal significance. For the significant associations, concordant estimates were basically suggested by weighted median, MR-Egger, MR-PRESSO, and MRlap.
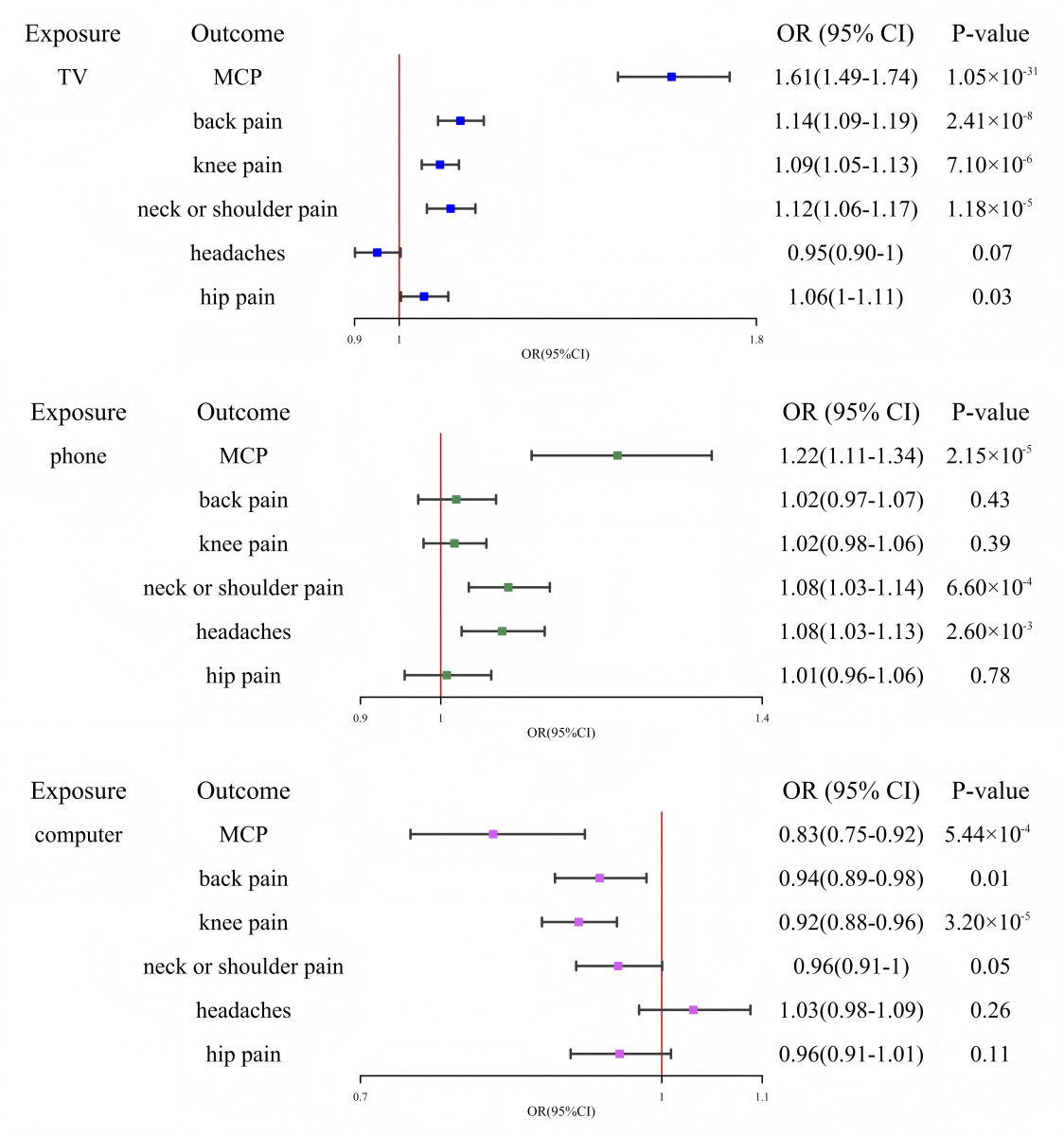 Figure 2. Mendelian randomization analysis of screen time and chronic pain based on the inverse variance weighted. MCP: multisite chronic pain; OR: odds ratio; TV: television.
Figure 2. Mendelian randomization analysis of screen time and chronic pain based on the inverse variance weighted. MCP: multisite chronic pain; OR: odds ratio; TV: television.
MRlap-corrected results in showed that time spent watching television significantly increased the risk of MCP (Pcorrected=3.57×10–30; ORcorrected=1.53, 95% CI 1.43-1.65), back pain (Pcorrected=8.46×10–6; ORcorrected=1.27, 95% CI 1.14-1.41), knee pain (Pcorrected=1.14×10–4; ORcorrected=1.22, 95% CI 1.11-1.36), and neck or shoulder pain (Pcorrected=6.99×10–4; ORcorrected=1.19, 95% CI 1.08-1.31). Length of mobile phone use significantly increased the risk of MCP (Pcorrected=1.04×10–4; ORcorrected=1.39, 95% CI 1.18-1.64), headaches (Pcorrected=.03; ORcorrected=1.34, 95% CI 1.04-1.74), and neck or shoulder pain (Pcorrected=.01; ORcorrected=1.55, 95% CI 1.1-2.17). In contrast, time spent using computer was negatively associated with the risk of MCP (Pcorrected=1.65×10–3; ORcorrected=0.81, 95% CI 0.71-0.92), back pain (Pcorrected=4.28×10–3; ORcorrected=0.83, 95% CI 0.73-0.94), and knee pain (Pcorrected=3.48×10–3; ORcorrected=0.83, 95% CI 0.73-0.94). Overall, the MRlap-corrected causal estimates were consistent in direction and statistical significance with the primary IVW results in , supporting the robustness of the findings against biases induced by sample overlap. Leave-one-out analyses in showed no outlying SNPs.
In the reverse MR analysis, MCP was used as the exposure, and different types of screen time were treated as outcomes. The F-statistics of IVs of MCP in are all greater than 10, indicating that the IVs are relatively strong. The results in indicated that MCP was positively associated with time spent watching television (P=4.8×10–7; OR 1.27, 95% CI 1.16-1.4) and length of mobile phone use (P=3.38×10–5; OR 1.29, 95% CI 1.14-1.45), while the association with time spent using computer (P=.61; OR 0.97, 95% CI 0.87-1.09) was not statistically significant. For other exposures, the analysis could not be conducted due to the limited number of available IVs or F-statistics below the conventional threshold of 10.
Independent Effect of Screen Time on Chronic Pain
showed that the causal effects of screen time on chronic pain based on IVW MVMR. The conditional F-statistics for both time spent using computer and length of mobile phone use is less than 10 in the MVMR results.
Discovery of Screen Time and Chronic Pain Genes Based on SMR Analysis
As the main analysis result, SMR was corrected by FDR and combined with the HEIDI test to screen for overlapping genes between exposure and outcome in 8 eQTL summary data. and provided the full results, including the exact PFDR and PHEIDI values for all tested genes after FDR correction. A total of 72 overlapping genes related to exposure and outcome were identified in , and the results showed that these overlapping genes originated from 3 exposures and MCP: 40 genes for time spent watching television and MCP, 26 genes for time spent using computer and MCP, and 6 genes for length of mobile phone use and MCP. In the SMR analysis, the Adipose Subcutaneous tissue had the most genes, while only one gene was found in the Brain Spinal cord cervical c-1.
Genetic Findings of TWAS-Based Screen Time and Chronic Pain
After Bonferroni correction, we examined genome-wide significant associations in and , followed by joint and conditional tests. and provided the results of the jointly significant genes. Then we identified 28 genes with overlapping exposures and outcomes in . No genes overlapping with the exposure were found in the hip pain for ≥3 months GWAS dataset.
Table 1. Transcriptome-wide significant genes identified by TWASa in screen time and chronic pain.TraitCross-tissue expressionGene (chromosome)Time spent watching television – back pain for ≥3 monthssCCA1Time spent watching television – MCPbsCCA2FUBP1 (1)
WDR47 (1)
PLEKHO1 (1)
FAM172A (5)
Time spent watching television – MCPsCCA3SUSD3 (9)
RPL35 (9)
RELA (11)
RMC1 (18)
SYPL2 (1)
SF3B4 (1)
ARPC5L (9)
PTPDC1 (9)
FAM53B (10)
Time spent watching television – knee pain for ≥3 monthssCCA2Length of mobile phone use – neck or shoulder pain for ≥3 monthssCCA3Length of mobile phone use – MCPsCCA3Time spent using computer – MCPsCCA2WDR47 (1)
RFTN2 (2)
NMT1 (17)
RMC1 (18)
FASTKD5 (20)
TM9SF4 (20)
Time spent using computer – MCPsCCA3SYPL2 (1)
CEP170 (1)
SCOC-AS1 (4)
Time spent using computer – headaches for ≥3 monthssCCA2
aTWAS: transcriptome-wide association study.
bMCP: multisite chronic pain.
By combining the results of SMR and TWAS analysis, we found that 7 overlapping genes (SYPL2, RMC1, FUBP1, ARPC5L, RFTN2, NMT1, and CEP170) were identified between exposures (time spent watching television and time spent using computer) and outcome (MCP) in and . In addition, we found that SYPL2 gene expression was associated with both time spent watching television and time spent using computer.
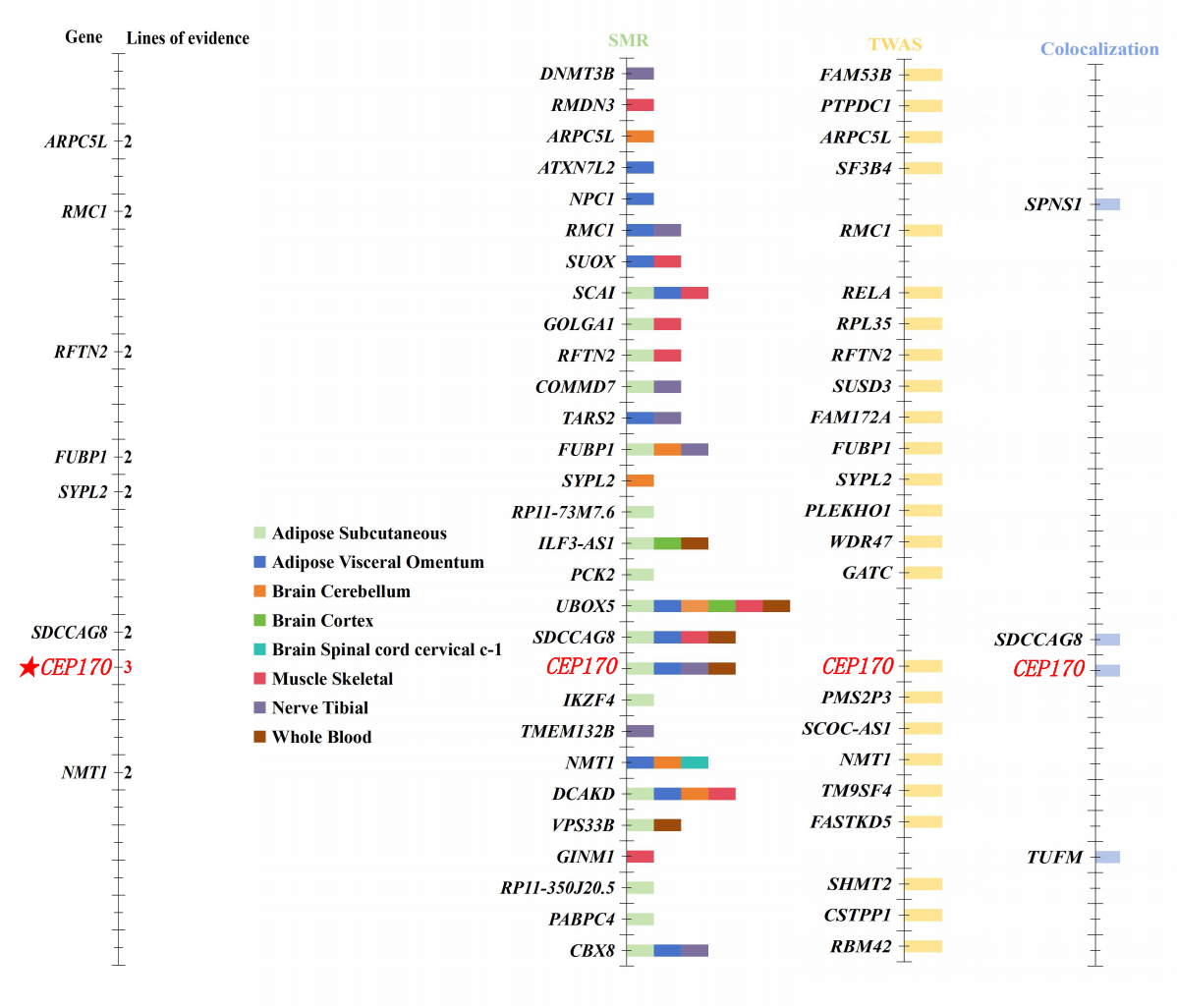 Figure 3. Results supported by genetic evidence. SMR: summary data–based Mendelian randomization analysis; TWAS: transcriptome-wide association study.
Figure 3. Results supported by genetic evidence. SMR: summary data–based Mendelian randomization analysis; TWAS: transcriptome-wide association study.
In , the panel on the far left shows genes supported by at least 2 lines of evidence. A total of 3 lines of evidence were used to support genes, with each column representing one type of supporting evidence. The SMR evidence shows different colors according to 8 different eQTL summary data. TWAS evidence is shown in light yellow and colocalization evidence is shown in light blue. CEP170 was supported by all analyses. ARPC5L, RMC1, RFTN2, FUBP1, SYPL2, SDCCAG8, and NMT1 were supported by 2 lines of evidence.
Colocalization Analysis of Shared Genetic Variation
Colocalization analysis identified multiple genes with moderate or strong support for colocalization signals in the shared genetic variation between screen time and chronic pain in . The results showed that 4 genes suggest a moderate support for colocalization (SPNS1, TUFM, SDCCAG8, and CEP170). showed that the 4 genes are overlapped between screen time and chronic pain.
Gene Discovery
As shown in , we presented the distribution of significant genes in each analysis method, and the results showed that the CEP170 gene stood out in the association analysis of “Time spent using computer” and MCP, receiving triple support from SMR, TWAS, and colocalization analysis (PPH4>.75). The signaling distribution of this gene involved 4 eQTL tissues: Adipose Subcutaneous, Adipose Visceral Omentum, Nerve Tibial, and Whole Blood.
DiscussionPrincipal Findings
This study delves into potential phenotypic associations and underlying genetic connections between screen time and chronic pain. The results show that screen time is associated with chronic pain. In the 2-sample MR results, time spent watching television and length of mobile phone use were significantly and positively associated with chronic pain, including MCP, back pain, knee pain, neck or shoulder pain, hip pain, and headaches. In contrast, time spent using computer inversely was negatively associated with MCP, back pain, and knee pain. It is particularly important to note that we still list the significant IVW results of exposure to the length of mobile phone use. Even though the effect value directions of the IVW and MR-Egger results are not consistent, it is consistent with the direction of our main analytical method in other methods. The statistical power of MR-Egger decreases for fewer IVs []. Therefore, we still take the results of IVW as the standard for the length of mobile phone use. In the reverse MR results, we found that there is a bidirectional positive correlation among time spent watching television, length of mobile phone use, and MCP. In the MVMR analysis, not all the conditional F-statistics were >10, suggesting the presence of weak instruments. Therefore, our interpretations were based on the 2-sample MR results. However, the inverse association between time spent using computer and MCP should be interpreted cautiously, as it stems from the 2-sample MR results. The lack of robust MVMR findings means we cannot rule out the potential influence of confounding factors. In addition, by integrating SMR, TWAS, and colocalization analysis, we identified an overlapping gene CEP170 associated with time spent using computer and MCP. These findings highlight the important role of screen time in the development of chronic pain.
Differential Associations Between Screen Time and Chronic Pain
Previous studies have shown a positive correlation between mobile phone use and neck pain [], and a strong correlation between watching television and back pain [], which is consistent with our research findings. In contrast, our research found that time spent using computer may have a protective effect on certain types of chronic pain, which differs from some studies that concluded, “longer computer time increases the risk of multi-site pain” [,]. This difference may be due to the study population, with earlier studies focusing on adolescents, while our analysis was conducted on adults. Due to continued musculoskeletal development, adolescents may be more susceptible to the negative physical effects of sedentary behavior.
Furthermore, 2 potential explanations may underlie the differential associations between time spent using computer and chronic pain, although there is no direct evidence available at present. One possible explanation is that the perception of pain is influenced by the allocation of cognitive resources; that is, when attention is occupied by other highly attractive stimuli, the perception of pain may be reduced [,]. According to the characteristics of the UK Biobank population (aged 40-69 years during 2006-2010) in this study [], the use of mobile phones and televisions was often associated with activities that had relatively low cognitive requirements and less attention input at that time. In contrast, even leisure-time computer use generally involved more cognitively demanding activities among middle-aged adults, such as reading, writing, online communication, or other interactive tasks. Research indicates that pain is less likely to enter conscious awareness when cognitive resources are occupied by goal-directed information maintained in working memory and when sustained attention is devoted to the task []. This indicates that computer tasks with high cognitive load may potentially reduce the pain experience through distraction. Moreover, it is also important to consider that individuals who frequently use computers tend to have higher educational attainment, higher income, and better overall health []. Given that individuals in nonmanual occupations tend to have a lower likelihood of experiencing chronic pain compared with those in manual labor occupations [,], part of the observed lower risk associated with time spent using computer may therefore reflect underlying socioeconomic or occupational factors rather than a sole reflection of the nature of computer-based activities themselves. This may explain why length of mobile phone use and time spent watching television were associated with a higher risk of pain, while time spent using computer showed a protective effect in this study.
Another possible explanation is that different types of screen time may affect pain perception by engaging the brain’s reward system to varying degrees. Dopamine is involved in pleasure, reward, and incentive behavior []. Although mobile phone and television use may induce pleasure, the limited interactivity prevents them from triggering dopamine release to the same extent as engaging in more goal-directed and cognitively engaging computer activities. Successfully completing such goals may elicit a sense of accomplishment. The reward system may be activated, promoting dopamine release, which has been proven to have analgesic effects [,]. Moreover, bidirectional association analysis suggests that MCP may influence the choice of screen behavior. People with MCP tend to increase passive and low-effort screen behaviors (such as watching television or casually browsing their mobile phones). This behavioral adaptation may contribute to a pattern of bidirectional reinforcement, where an increase in passive activity further restricts physical movement and may exacerbate pain. However, we emphasize that these explanations are speculative, as direct evidence is currently lacking.
The Potential Mechanisms by Which CEP170 Contributes to Screen Time and Chronic Pain
Leveraging multiomics approaches, we identified CEP170, whose cis-regulated expression may contribute to the biological mechanisms between time spent using computer and MCP. In SMR results, the CEP170 gene expression level was positively correlated with MCP but negatively correlated with time spent using computer. This aligns with our MR results, where time spent using computer was associated with a lower risk of MCP. One possible explanation is that CEP170 may influence behavioral patterns related to screen time, where individuals with higher gene expression tend to spend less time on the computer, which in turn is associated with increased MCP risk. Although its colocalization results suggest a moderate support for colocalization, CEP170 was detected in all analytical methods.
CEP170 is located at the centrosome and spindle microtubules and participates in microtubule organization and assembly [,]. Additionally, CEP170 plays an important role in supporting ciliary homeostasis []. Cilia may potentially play a central role in cell signaling, and recent animal experiments have further revealed that cilia have key regulatory functions in controlling mechanical nociceptive thresholds and inflammatory and neuropathic pain []. The SMR results show that CEP170 exhibited significant signals in multiple eQTL tissues, including Adipose Subcutaneous, Adipose Visceral Omentum, Nerve Tibial, and Whole Blood. This indicates that CEP170 may be expressed in these tissues and may contribute to the biological mechanisms behind the observed associations. A large UK Biobank study revealed that abdominal adipose tissue (including visceral fat and subcutaneous fat) was associated with chronic musculoskeletal pain. It suggested that excessive and ectopic fat depositions may be involved in the pathogenesis of multisite and widespread chronic musculoskeletal pain []. This is likely attributable to the chronic low-grade inflammation driven by accumulated visceral fat, which can sensitize peripheral nerves and promote MCP [,]. In line with this, our SMR analysis found that CEP170 expression in subcutaneous and visceral adipose tissue is associated with MCP. Given the established importance of microtubules in lipid metabolic homeostasis [,], we hypothesize that CEP170 may potentially protect against MCP by enhancing microtubule stability in adipose tissue. This mechanism might potentially constrain adipose-derived inflammatory signaling, thereby possibly alleviating peripheral nerve sensitization and lowering MCP risk. However, the current results only provide preliminary genetic clues. Direct links remain unclear and more functional studies, especially tissue-specific experiments, are needed in the future to clarify the potential contribution of CEP170 to pain pathways.
Strengths and Limitations
Our research has several advantages. First, we integrated a variety of analytical methods to duplicate our findings and strengthen the robustness of our results. Second, we leveraged large-scale GWAS data from the UK Biobank, ensuring a robust analysis with broad generalizability. Third, by identifying overlapping genes and potential biological pathways, our study provides new genetic insights into the association between screen time and chronic pain, which, despite limited evidence, may inform future research in this field. Finally, our study considered different types of screen time separately, which allows for a more nuanced understanding of their different effects on chronic pain. These findings may serve as a useful reference for subsequent studies on the genetic and epidemiological links between screen time and chronic pain.
Although this study provides new insights, there are still some limitations. First, using data from the same sources in multiple analyses may introduce the bias of the winner’s curse, potentially inflating effect sizes or significance levels. Replication in fully independent datasets is necessary to confirm the discovery. Second, our analyses were restricted to European populations, which may limit generalizability to other populations with different screen use habits and pain reporting. Third, the lack of detailed data on screen use posture, activity type, and behavior patterns may limit the depth of causal reasoning. Future studies could incorporate longitudinal and behavioral data to better clarify the mechanisms and causal pathways. Fourth, as both exposures and outcomes are self-reported, recall and measurement bias may lead to misclassification and reduce precision. Self-reported pain may not capture clinical heterogeneity, so future studies using clinically validated phenotypes are needed. Fifth, due to the weak strength of IVs, we were unable to adequately control for crucial potential confounding factors, such as socioeconomic status and educational attainment. Consequently, the observed protective association between “time spent using computer” and chronic pain might be partially attributable to residual confounding by socioeconomic status and related factors. Sixth, reverse MR could not be performed for the outcomes of back pain, knee pain, neck or shoulder pain, headaches, and hip pain due to limited IVs, limiting the assessment of reverse causality. In addition, the smaller sample size for hip pain may have limited statistical power, contributing to borderline significance in the 2-sample MR analysis and precluding reverse MR for this phenotype. Seventh, environmental exposure, such as air pollution, was not taken into account in this analysis. Particulate matter can affect inflammatory and stress-related biomarkers involved in chronic pain [-]. Future studies should integrate genetic and environmental data to clarify these relationships. Eighth, the colocalization signal for CEP170 is not the strongest, and direct evidence is lacking. Therefore, its role remains speculative and warrants further investigation. Finally, this study lacks validation in large surveys or independent cohorts, highlighting the need to combine genetic and epidemiological studies in future research.
Conclusions
This study provides evidence that reveals an association between screen time and chronic pain. We found the CEP170 gene might contribute to the shared biological mechanism between time spent using computer and MCP risk. Future studies should further validate this association and clarify the functional role of CEP170 in the development of chronic pain.
The authors would like to thank the participants and investigators involved in the GWASs used in this study.
This work was supported by the Hainan Provincial People’s Hospital Scientific Research Start-up Fund (grant number YJRC2025009).
The code used in this study is available from the corresponding authors on reasonable request. The GWAS summary statistics data used in this study are available from IEU OpenGwas and publicly available GWAS. The eQTL summary data for GTEx used in the SMR analysis are available in the public database []. Precomputed sCCA weights for GTEx v8 used in this study are available in the public database []. The eQTL data used in the colocalization analysis are available from the eQTLGen Consortium [].
CX and ZL contributed equally as corresponding authors. JJ, CP, and JC contributed equally to this work and share first authorship. JJ and CX conceived the study. JJ and CP performed the data analysis and interpretation. JJ and CP wrote the manuscript. JC, CP, and JJ critically revised the manuscript. CY, CP, JC, and CX provide additional methodological guidance and technical support. CX and ZL supervised the study and were responsible for overall project administration. All authors reviewed and approved the manuscript.
None declared.
Edited by A Coristine; submitted 29.May.2025; peer-reviewed by J Dolcini, Y Zhu; comments to author 24.Oct.2025; accepted 24.Dec.2025; published 09.Feb.2026.
©Jiahui Jiang, Chunyan Pu, Jiarui Cai, Chuan Yu, Zhenmi Liu, Chenghan Xiao. Originally published in the Journal of Medical Internet Research (https://www.jmir.org), 09.Feb.2026.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work, first published in the Journal of Medical Internet Research (ISSN 1438-8871), is properly cited. The complete bibliographic information, a link to the original publication on https://www.jmir.org/, as well as this copyright and license information must be included.