

At the completion of this article, the reader should…
• Recognise common concerns and current evidence regarding the visual risks of VR use, particularly in children.
• Apply current usage guidelines and age-based recommendations for safe VR use in paediatric populations.
• Evaluate the potential of VR in myopia management, including its capacity to simulate distance vision and influence ocular growth.
 Hayley McDonald.
Hayley McDonald.
Hayley McDonald
BMedSci(VisSci), MOpt,
SpecCert(Paediatrics)
Lecturer (optometry)
College of Nursing and Health Science
Flinders University, Adelaide,
South Australia
With VR use on the rise – especially among children – optometrists need to understand its risks and potential in clinical care. Hayley McDonald, lecturer in optometry at Flinders University, outlines the visual impacts of VR and explores its emerging applications in amblyopia, vision therapy, and myopia management.
Virtual reality (VR) is no longer a futuristic concept; it’s rapidly becoming part of everyday life for many Australians.
With an increasing number of consumers, especially younger demographics, embracing VR technology, it’s crucial that optometrists stay informed about both the potential risks and clinical opportunities associated with the use of VR technology.
As primary eyecare providers, we should recognise VR’s visual implications as well as its emerging role within our profession.
Defining virtual reality
Virtual reality refers to an immersive, simulated three-dimensional environment, typically experienced through a headset. It is part of the broader category of extended reality (XR), which also includes augmented reality (AR), where digital elements overlay the real world (e.g. Pokémon Go), and mixed reality (MR), where users physically interact with digital elements (as seen with Iron Man’s virtual interfaces).
While the first mainstream VR devices appeared in the 1990s, today’s systems offer significantly improved visual content, used across gaming, entertainment, education, and increasingly, healthcare.
Potential risks of virtual reality use
Understandably, many parents and professionals alike are concerned about VR’s impact on vision, particularly in children.
A 2017 US-based survey revealed that 60% of parents are concerned about the potential effect of virtual reality on their children’s health.1
Vision and physical health
To date, there have been several studies examining single-session use of VR and its impact on eyesight and binocular vision.
These studies reported minimal or no changes in visual acuity, refractive error, ocular alignment, gaze stability, or stereopsis in both paediatric and adult participants.2,3
However, long-term data is limited, and current evidence does not yet address the cumulative effects of regular or prolonged use of VR devices.
Additionally, VR headsets are typically designed for adult users. In children, poor fit due to smaller interpupillary distances or skull dimensions may lead to short-term discomfort or, in rare cases, longer-term anatomical changes.
One such case, reported in 2022, describes a 10-year-old boy who developed cartilaginous and bony nasal changes after using an ill-fitting headset for one hour daily over the course of a year.4
Cognitive and psychological development
The immersive nature of VR poses challenges, particularly for younger users who may struggle to distinguish the realistic virtual environments from reality.
Concerns have been raised about potential impacts on spatial cognition, technology dependency, anxiety, and social development.
While the current evidence remains inconclusive, many psychologists and educational professionals recommend cautious, limited use among children.5
Cybersickness
The most common short-term adverse effect associated with VR is cybersickness, a condition resembling motion sickness, triggered by conflicting visual, vestibular, and proprioceptive inputs.
Studies suggest that children do not appear to be more susceptible to cybersickness than adults, and symptoms such as nausea, headache, and eye discomfort occur at similar rates to traditional screen use (e.g. television).6
A 2024 meta-analysis by Bexson et al. found no significant evidence of harm associated with virtual reality use in children for any of the categories discussed above.7
However, the authors emphasised that most of the studies reviewed reported adverse effects only as secondary outcomes, often using heterogeneous and non-standardised reporting methods.
Importantly, they cautioned that “absence of evidence is not evidence of absence” and while preliminary findings are reassuring, ongoing research is needed to establish clearer safety parameters for younger users.7
Clinical applications of virtual reality
Despite these concerns, VR also offers exciting clinical opportunities in optometry.
Its ability to deliver separate images to each eye, provide a wide field of view, control lighting conditions, and create a fully immersive experience means that it has the potential for valuable treatment interventions.
Amblyopia treatment
VR is emerging as a promising adjunctive therapy for amblyopia. Instead of relying solely on traditional patching, which can be challenging for compliance, VR-based interventions allow for engaging, game-like environments that stimulate binocular vision.
These systems typically present differing, yet coordinated, images to each eye, strengthening the amblyopic eye while promoting binocular fusion.
Some platforms also adjust for strabismic deviations, including horizontal, vertical, and torsional misalignments.
A recent meta-analysis reported an additional 3.5 logMAR letter improvement in patients receiving VR-assisted therapy alongside conventional treatments, compared to patching or penalisation only.8 The greatest benefit was observed in children under seven years old.
Currently, VR is mainly being studied as a supplemental therapy in addition to patching or penalisation, rather than a standalone treatment.
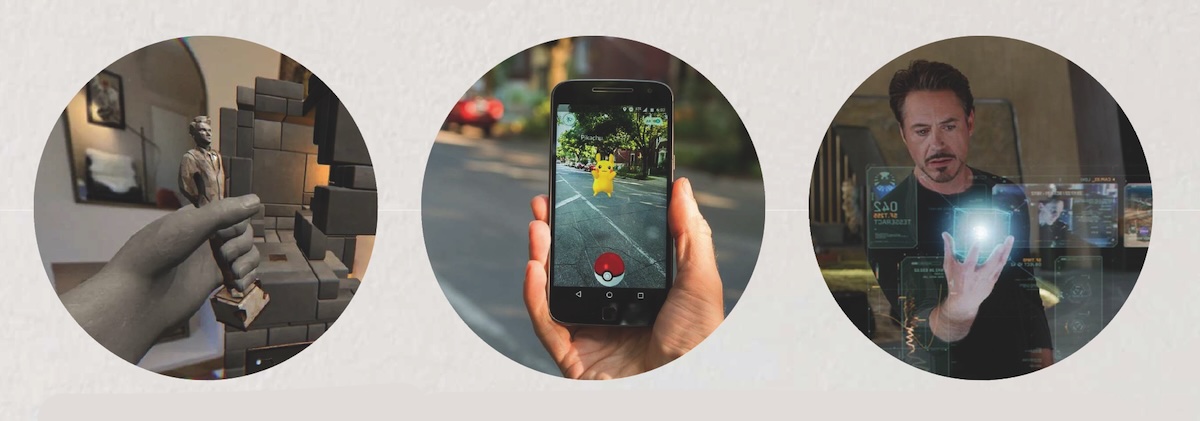 Figure 1. Examples of extended reality (XR). Left to right: virtual reality (VR), augmented reality (AR) and mixed reality (MR). Image: Hayley McDonald.
Figure 1. Examples of extended reality (XR). Left to right: virtual reality (VR), augmented reality (AR) and mixed reality (MR). Image: Hayley McDonald.
Vision therapy
VR technology is being increasingly explored in vision therapy, particularly in the management of binocular vision disorders such as convergence insufficiency and accommodative dysfunction.
VR platforms provide an immersive and controllable environment ideal for training vergence and accommodative systems.9
Through real-time manipulation of stimulus distance and depth cues, VR exercises can replicate and intensify vergence demands.
Many programs require users to track objects moving in three-dimensional space, promoting precise binocular coordination. Similarly, accommodative function can be trained using dynamic changes in virtual object distance and clarity, mimicking real-world visual demands in a controlled, measurable format.
Early clinical studies and expert reviews, including Levi (2023), support the potential of VR to improve convergence facility, reduce symptoms, and enhance accommodative response.10
The engaging nature of VR is particularly advantageous for younger patients or those who struggle with traditional vision therapy compliance.
In addition to binocular vision therapy, VR is gaining traction in the rehabilitation of patients with visual deficits following neurological injury, such as stroke or traumatic brain injury.
Patients with hemianopia, visual neglect, or oculomotor dysfunction may benefit from VR-based programs designed to promote scanning strategies, enhance visual attention, and retrain saccadic and pursuit eye movements.
A 2018 Cochrane Review by Laver et al investigated the use of VR as an intervention for improving upper limb function. They concluded that VR was no more beneficial than conventional therapies, but that there was further improvements when implemented in addition to usual care, increasing the overall therapy time.11
As with many medical applications of VR, it appears that we will not be reinventing the wheel, but instead making it more efficient.
Myopia management
One of the most interesting potential applications of VR in optometry, in my opinion, is in the myopia management space.
While VR headsets place screens in close proximity to the eye, the visual system is not necessarily stimulated in a near-focus manner.
Unlike smartphones or tablets, where content is fixed at a near point, VR displays can simulate optical infinity through lens design and software rendering.
In addition to focal length manipulation, VR environments offer precise control over visual parameters such as luminance, contrast, wavelengths, and depth cues. These variables have all been implicated, to varying degrees, in ocular growth.
Preliminary research has shown that short-term use of VR may lead to increased choroidal thickness, a physiological marker correlated with reduced eye growth.12
Although this is a short-term finding, it raises the possibility that VR could be used as a therapeutic tool to mimic the protective effects of outdoor light exposure or to provide structured visual tasks that discourage axial elongation.
Future investigation is required to determine whether VR use can produce a measurable and sustained reduction in axial elongation over time. Questions also remain about safe dosing (duration and frequency), and optimal display settings.
Guidelines and recommendations
Most VR headset manufacturers advise that their devices are not suitable for children under the age of 12 or 13. This aligns closely with the guidance provided by Australia’s eSafety Commissioner.13
These age-based recommendations are largely driven by two key concerns: the physical design of the headsets, which are typically intended for adult facial anatomy and interpupillary distances, and the current absence of robust, long-term data regarding the impact of VR use on the developing visual system.
In terms of usage guidelines, VR is generally subject to the same principles that apply to other forms of digital media consumption in children.
Currently there are no specific VR-related standards. Recommendations include age-appropriate content selection, time limits to reduce the risk of visual fatigue and eye strain, and regular breaks to support healthy visual habits. Parental supervision and the use of content filters or built-in safety features are also encouraged to ensure a safe and developmentally appropriate user experience.
Optometrists can take a proactive approach by discussing safe VR use with families during consultations, especially for children presenting with digital eye strain, binocular vision anomalies, or myopia progression.
Future research and opportunities
Emerging areas of investigation include:
• Longitudinal studies on the impact of VR on visual development.
• Optimisation of VR systems for paediatric use, including adjustable interpupillary distances and lightweight headsets.
• Development of VR tools for low-vision rehabilitation and patient education.
• Detailed investigation of the efficacy of VR as a vision therapy tool.
• Use of artificial intelligence to customise VR therapeutic environments in real time.
As the technology evolves, optometrists may also see new opportunities in remote consultation and home-based vision therapy delivered via VR platforms.
Virtual reality presents both exciting opportunities and important challenges for eyecare. As optometrists, our role is to balance innovation with evidence-based care.
While short-term use appears to pose minimal risk, caution is warranted until long-term data becomes available, especially for paediatric patients.
Clinically, VR offers unique tools for amblyopia treatment, vision therapy, and potentially myopia control, tools that can improve compliance, engagement, and therapeutic outcomes.
As VR becomes further embedded in both entertainment and healthcare, optometry is well-positioned to lead the way in ensuring that the visual needs of our youngest Australians are met safely and effectively.
References:
1.Aubrey, J. (2018) Virtual reality 101, commonsense.org. Available at: https://www.commonsensemedia.org/sites/default/files/research/report/csm_vr101_final_under5mb.pdf
2. Tychsen, L. and Foeller, P. (2020) ‘Effects of immersive virtual reality headset viewing on young children: Visuomotor function, postural stability, and motion sickness’, American Journal of Ophthalmology, 209, pp. 151–159.
3. Turnbull, P.R. and Phillips, J.R. (2017) ‘Ocular effects of virtual reality headset wear in young adults’, Scientific Reports, 7(1).
4. Nasrollahi, T.S., Lee, M.K. and Liu, G.C. (2022) ‘Adaptive nasal bone remodeling secondary to chronic virtual reality headset use’, American Journal of Otolaryngology, 43(5), p. 103587.
5. Kaimara, P., Oikonomou, A. and Deliyannis, I. (2021) ‘Could virtual reality applications pose real risks to children and adolescents? A systematic review of ethical issues and concerns’, Virtual Reality, 26(2), pp. 697–735.
6. Oh, H. and Son, W. (2022) ‘Cybersickness and its severity arising from virtual reality content: A comprehensive study’, Sensors, 22(4), p. 1314.
7. Bexson, C., Oldham, G. and Wray, J. (2024) ‘Safety of virtual reality use in children: A systematic review’, European Journal of Pediatrics, 183(5), pp. 2071–2090.
8. Shao, W. et al. (2023) ‘Effects of virtual reality on the treatment of Amblyopia in children: A systematic review and meta-analysis’, Journal of Pediatric Nursing, 72, pp. 106–112.
9. Li, S et al (2022) ‘Virtual reality-based vision therapy versus OBVAT in the treatment of convergence insufficiency, accommodative dysfunction: a pilot randomized controlled trial’. BMC Ophthalmol. 2022, 22(1).
10. Levi, D.M. (2023) ‘Applications and implications for extended reality to improve binocular vision and stereopsis’, Journal of Vision, 23(1), p. 14.
11. Laver, K.E. et al (2017) ‘Virtual reality for stroke rehabilitation’, Cochrane Database Syst Rev, 11(11).
12. Xu, Z. et al. (2024) ‘Effect of virtual reality-based visual training for Myopia Control in children: A randomized controlled trial’, BMC Ophthalmology, 24(1).
13. eSafety Commissioner (2024) Virtual reality (VR) eSafety, eSafety Commissioner. Available at: https://www.esafety.gov.au/parents/resources/gift-guide/virtual-reality-vr.