
Solutions to the ongoing crisis in emergency departments, the importance of a trusted, safe medication management service for Aboriginal and Torres Strait Islander patients, and the possibilities of dance for science communications are among topics covered in The Health Wrap this week.
Writing from Colorado, Adjunct Associate Professor Lesley Russell continues to document the wide-ranging impacts of the Trump Administration upon health, and also takes a deep dive into health workforce policies in Australia.
The quotable?
The current focus [of workforce policy] is on what’s most visible, what’s perceived as urgent, rather than what’s systemic and sustainable.”
Lesley Russell writes:
The weather here in Colorado continues to be the key topic of conversation – we have had a few significant snowfalls, but these are quickly followed by very warm temperatures that swiftly melt the snowpack, leaving icy, muddy patches everywhere.
This coming week we are expecting to get hit by what is being described as “an exceptional, long-duration, and record-breaking March heatwave” centred across the American southwest.
We are getting some skiing in, but the runs are increasingly bare, and many days we seek our exercise by snowshoeing – or even hiking through the mud.
 Snowshoeing on Willow Trail at Breckenridge
Snowshoeing on Willow Trail at Breckenridge
The other key topic of conversation here is the cost of petrol/gasoline. It’s one way everyone – regardless of politics – is aware of the cost of Trump’s Middle East war.
Our local newspaper, which is widely read, has little focus on what is happening in Washington, Iran, Lebanon and the Straits of Hormuz.
This past week the topics covered have included: the impact of the weather on the local (mainly tourist) economy; the push to get the US Forest Service to accelerate fire mitigation efforts; farmers’ compensation claims for wolf damages to their livestock; monitoring high-altitude lakes for the impacts of climate change and pollutants on ecosystems; and how Summit County is addressing the unique health and healthcare challenges facing older adults living at high altitudes.
Costs of war and healthcare
The first week of President Trump’s war against Iran is estimated to have cost US taxpayers of somewhere around US$11 billion. The final costs will be billions more.
Trump came into office promising to reduce prices and instead has enacted a bunch of economic policies and now a war that have increased prices. Everyone knows how much petrol prices have risen since the war started.
High healthcare costs will be a central feature of the upcoming midterm elections. Americans have been finding their health insurance premiums and their bills harder and harder to afford. These costs rank as the top financial worry for adults and their families.
Two new Gallup polls find:
About half of middle-income households have delayed a major life event because of medical costs.
One-third of Americans skip meals or other needs to afford healthcare.
About half of middle-income households said they have delayed a major life event because of medical costs.
Nearly one in ten Americans reported postponing retirement in the past four years due to healthcare costs.
Six percent said they postponed having or adopting a child.
 https://www.axios.com/2026/03/12/healthcare-costs-america-survey-sacrifices
https://www.axios.com/2026/03/12/healthcare-costs-america-survey-sacrifices
While billions of tax dollars are allocated to the new conflict in the Middle East, the domestic situation is in a crisis for millions of households.
A single Tomahawk missile costs enough to cover the annual Medicaid expenses of 775 children or provide school lunches for 3,600 more, according to data from the Center for American Progress. You can read more here.
And then there’s the dreadful, almost unimaginable, healthcare costs for the victims of this war which is now reaching 14 countries.
See Dr Richard Horton’s opinion piece in The Lancet: The human consequences of Epic Fury.
Gutting science and trust
The situation for science and scientists in Trump’s America is becoming increasingly untenable.
Given the way science works (or should work) internationally, this has direct impacts on Australia – on the ability to have shared research projects, on the exchange opportunities for graduates and on the levels of misinformation, disinformation and distrust that are promulgated internationally.
In total, science agencies saw nearly 95,000 departures. Agencies that oversee climate science and adaptation have been particularly hard hit.
The New York Times highlighted some examples of what the cuts have done to government climate work here.
The paper also ran an article on what happened to a Harvard researcher who lost his NIH grants to study healthy ageing.
KFF Health News recently ran an article about the work left undone as six senior scientists were forced out of their laboratories at the National Institutes of Health.

A recently-published peer-reviewed paper assesses the impacts on Americans’ pulmonary health, across the life course, of policies proposed or enacted in the first year of the second Trump Administration.
These policies include:
The rollback of environmental protections and reduction in subsidies for clean energy production that will worsen air quality and accelerate climate change.
Cuts at the Centers for Disease Control and Prevention (CDC) which will disrupt occupational health protections and tobacco and asthma control efforts.
The embrace by the Department of Health and Human Services (HHS) leadership of anti-vaccine theories that will drive vaccine-preventable illnesses.
The termination of federally-funded research grants, including some focused on respiratory diseases, that will slow medical progress.
Sweeping disruptions to global health aid that will impede global tuberculosis control.
 https://x.com/awgaffney/status/2032441786170319298?s=58
https://x.com/awgaffney/status/2032441786170319298?s=58
Even though Congress rejected cuts by the Trump Administration to the 2026 NIH budget and passed a funding bill more than a month ago, that money isn’t yet making it into the hands of researchers, experts say.
A key reason – as first reported by Nature – is that the Office of Management and Budget (OMB) hasn’t granted the agency spending authority to fund awards.
And it seems that applications are still being screened for alignment with agency priorities, which could be leading to delays.
While the NIH has frequently said there are no “banned” words, there is apparently an AI system that is used to check grants to make sure that they’re aligned with agency priorities.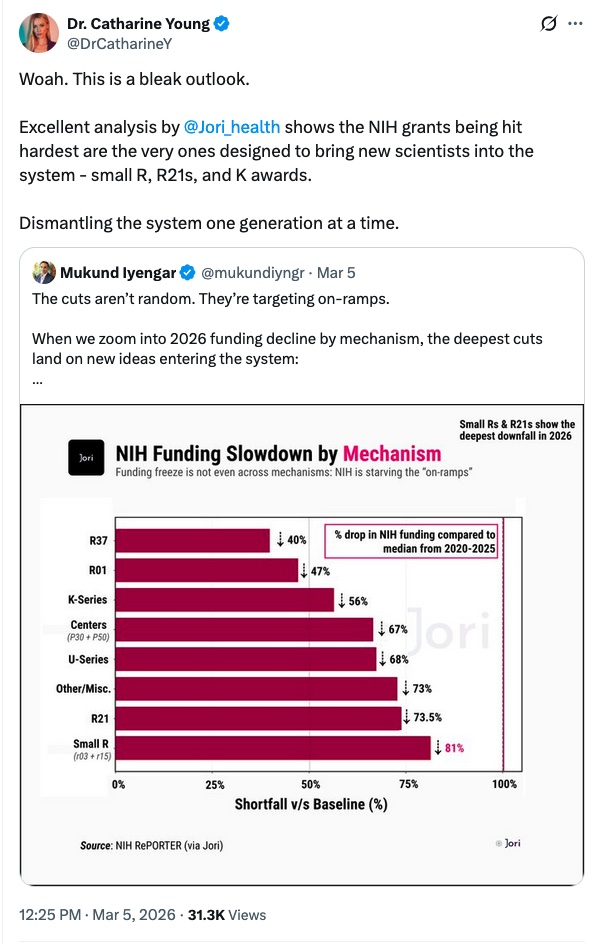

I have no indication as to whether or how the threats initially made to overseas universities and scientists, including that funds would not be made available to institutions and projects that support Diversity, Equity, and Inclusion (DEI) issues, have been implemented and are affecting Australian-based research.
A new poll from the Annenberg Public Policy Center at the University of Pennsylvania shows that public confidence that career scientists at federal health agencies such as the Centers for Disease Control and Prevention (CDC), the National Institutes of Health (NIH) and the Food and Drug Administration (FDA) are providing the public with trustworthy information about matters concerning public health is significantly higher than confidence in the Trump-appointed leaders of those agencies.
Public trust in the CDC, FDA, and NIH dropped significantly from 2024 (when it was around 75 precent) to 2025 (when it was 67 percent) and it has fallen again in 2026 (to 61 percent).
People have greater trust in major health and science associations outside government – such as the American Heart Association, American Academy of Pediatrics, American Medical Association, and National Academy of Sciences – than in US health agencies.
Only 38 percent of American adults are confident Secretary of HHS Robert F Kennedy Jr is providing trustworthy information on public health. This is considerably lower than the confidence people say they had in Dr Anthony Fauci (54 percent), former head of the National Institute of Allergy and Infectious Diseases, who was much maligned by the Trump Administration, when he was in office.
Emergency crisis continues
Recent reports highlight that there is much work to be done to address what can rightly be called the crisis in the Emergency Departments (EDs) of Australia’s public hospitals – the very EDs we all depend on when there is a accident or a medical emergency.
I see nothing in the recently announced new funding for the National Health Reform Agreement that will effectively address this, although the topic was a matter of concern during the Federal/State and Territory negotiations.
The recently released annual Public Hospital Report Card from the Australian Medical Association shows that overall performance across the country for EDs was worse in 2024-25 compared with a decade earlier.
The proportion of people in all triage categories who completed their emergency presentation – seen, treated, discharged or admitted – in four hours or less fell to a record low of 53 percent, down from 73 percent in 2015-16. No jurisdiction completed more than 61 percent of their ED presentations within four hours.
The AMA (which has its own agenda here, but whose data is always first class) attributed this failing to a “fundamental capacity problem, one that won’t be fixed without specific attention,” as the federal president, Dr Danielle McMullen, wrote in her introduction to the report.
Health Services Daily has a good analysis of this report, available here.
This report came just days after the December quarter report from the NSW Bureau of Health Information (BHI) into NSW hospitals. This highlights that even though NSW presents some of the best national data (as per the AMA report), the system is in crisis.
Treatment started “on time” for 66 percent of patients in that quarter and the median time from arrival to leaving the ED was three hours and 46 minutes, up 12 minutes compared to a year earlier.
That’s the good news. But almost 80,000 people were categorised as leaving the ED without completing treatment.
NSW Health says that of this figure, two-thirds of patients were treated but had not received their discharge summaries, while a third chose not to wait to be treated. Neither outcome is good – for patients or their GPs.
The NSW AMA president Dr Kathryn Austin commented: “This is highly concerning given almost 35 percent of those were in triage category 3 – needing urgent care for potentially life-threatening conditions and unsuitable to be treated at an urgent care centre.”
(We don’t know how many of these patients were seeking help for mental health issues.)
NSW Health Minister Ryan Park has conceded the system is under strain and blames “bed block” (sometimes called access block) as a major factor exacerbating the problem, which he then blames on the Federal Government.
“We can’t have a situation where we’re seeing 50 percent more patients languishing in our hospitals because they can’t get access to an aged care bed or they can’t get NDIS support. That’s not a system that’s working when it’s a two-funded system,“ he told ABC News.
Bed availability per person in public hospitals has stagnated in recent years. And Minister Park is correct in stating that the lack of aged care and NDIS (and rehabilitation) resources are significant contributors to bed block.
It is estimated that some 3,100 aged care patients are currently stuck – inappropriately – in hospital beds across the country.
I have tried unsuccessfully to find data on bed occupancy rates in public and private hospitals in recent years, without success. Traditionally, a target figure of 85 percent has been suggested as an optimal occupancy level to achieve good patient flow.
But I did find a very interesting paper published last month The Medical Journal of Australia, which looked at the effect of hospital occupancy levels on inpatient and ED flow rates, ED length of stay, and bed block in public hospitals in Queensland.
The study found a strong correlation between hospital bed occupancy and ED access performance, with higher hospital occupancy correlating with longer ED stays and decreased adherence to performance indicators.
But there is also evidence that staffing and other operational pressures play a role: significant disparities in hospital operations were observed between weekends and weekdays, with weekday admissions and discharges up to three times higher than weekends.
In 2022 the Australasian College for Emergency Medicine (ACEM) commissioned the Sax Institute to review published literature on solutions to bed block. This paper was presented to a committee of the NSW Parliament.
One of the solutions proposed was the development of opportunities to improve acute health care through the use of virtual care systems. It’s easy to see how this could make a difference for frail patients in aged care.
In 2023 the ACEM put out a position statement on ED overcrowding. The recommendations included adopting a whole-of-hospital and whole-of-system approach to the issue.
And I’m reminded that back in 2019 I wrote an article titled Tackling the Emergency Department crisis: Some “what if?” scenarios. I think it has some ideas that are still worth considering, especially those that address emergency mental health needs.
To the suggestions in the article (now some seven years old) I would add:
The recommendations from ACEM cited above about virtual care systems and a whole-of-hospital approach.
More funding for rehabilitative, step-down and geriatric care (as was once include in the NHRA under the Rudd Government).
More research and resources on the times when a hospital is not the answer. This applies particularly to the needs of the homeless, the elderly, people living with disabilities, and those who immune-compromised.
More research and policy development and public awareness on the interactions between EDs and Urgent Care Clinics. This particularly in light of the data from the BHI report that shows in October–December 2025, the number of ED attendances was also the highest since 2010.
Workforce issues
It makes sense that a discussion of how to address problems in public hospitals is followed by a section on workforce issues. One of my most-used aphorisms is that there is no healthcare reform without workforce considerations.
The National Medical Workforce Strategy 2021–2031 is now halfway through its lifespan. On the webpage headed Progress in Implementing the National Medical Workforce Strategy 2021–2031, there is only a document on Analysis of Locum Use on the Medical Workforce and a statement that the Department of Health, Disability and Ageing (DoHDA) is implementing several Australian Government–led actions in the strategy.
These include: progressing governance arrangements for a new joint planning and advisory body; developing a Hospital Registrar and Career Medical Officer Framework; and research the use of locums in the medical workforce.
Elsewhere, on a webpage that has not been updated since October 2024, I find that the Medical Workforce Advisory Collaboration (MWAC) was established in August 2024. There are communiques from five meetings held since then.
MWAC provides its advice to government through the Health Workforce Taskforce. There are updates from the HWT for 2024 and 2026 – but nothing for 2025.
Somehow I don’t get the idea that reforming and boosting the healthcare workforce is a priority for the Federal Government or DoHDA.
Yet it should be, as highlighted by a paper published by MJA last year that examined Federal health workforce policy in Australia and its implications.
This analysis found that Australia has 121 health workforce policies but no national plan. There were 35 rural health workforce policies, 22 for aged care and 19 for the Aboriginal and Torres Strait Islander health workforce, but none focused on public health or emergency care.
The authors concluded: “The absence of a unified federal health workforce strategy exacerbates policy fragmentation, undermining coordinated workforce planning and equity. Adopting a consistent policy nomenclature and reducing imbalances in strategic focus are critical for effective health workforce reform.”
The authors of this paper wrote it up for The Conversation (you can read their article here).
Two things stood out for me:
As so many of us have done for so long, they bemoan the loss of Health Workforce Australia and its independent expertise. There’s now no effective mechanism to ensure strategies and policies work together coherently and that all professions or service areas are covered.
Without this national (and independent) coordination, workforce policy and planning risks being reactive, inconsistent, and susceptible to political cycles. The current focus is on what’s most visible, what’s perceived as urgent, rather than what’s systemic and sustainable.
First Nations health
Two recent papers highlight how much more work there is to be done around preventive health issues for First Nations people in Australia.
The need to accelerate the elimination of cervical cancer in Aboriginal and Torres Strait Islander women
Australia is held out as an example of the success of vaccination against Human Papillomavirus (HPV) to protect against cervical and some other cancers. About 86 percent of 15-year-old girls and 83 percent of 15-year-old boys were fully immunised against HPV in 2023, and Australia is projected to become the first country to eliminate cervical cancer within the next decade.
But those great numbers hide the fact that, under current vaccination and screening rates, cervical cancer elimination among Aboriginal and Torres Strait Islander women is not projected to occur until 2047. (The national strategy aims to eliminate cervical cancer for all women by 2035 and this is well ahead of schedule).
A modelling study recently published in The Lancet shows that a one-off large-scale screening initiative that reached all unscreened Aboriginal and Torres Strait Islander women, and sustained efforts thereafter, could achieve elimination by 2036, aligning with national targets and setting a precedent for global efforts.
I quote the paper’s conclusion on how important a culturally sensitive, community-led screening effort is to achieving this goal:
“This could be achieved through Indigenous community-led approaches that prioritise cultural safety and impact, such as self-collection or point-of-care testing, delivered via community co-designed pathways.
“It is likely that these broad findings, specifically that reaching never screened individuals will have the greatest effect on expediting elimination, would also apply to other populations that have also experienced barriers to screening (such as LGBTQ+ populations, multicultural populations, those with a disability, who are intersex, or who live in rural or remote areas) but where there are limited data to support direct modelling.”
Ending rheumatic heart disease in Aboriginal and Torres Strait Islander communities
The ongoing levels of rheumatic heart disease (RHD) in Aboriginal and Torres Strait Islander communities – some of the highest in the world – has been a national shame for decades.
Australian Institute of Health and Welfare data from 2024 report that Indigenous communities accounted for 78 percent of all RHD cases, underscoring the critical health, housing and socio-economic disparities that confront these communities, especially those in remote areas.
The RHD Endgame Strategy seeks to eliminate RHD by 2031. A recent paper published in The Lowitja Journal finds that, to reach this goal, collective and urgent action is required that prioritises Indigenous-led and community-based prevention programs.
A focus on addressing health inequities and the political, social and cultural determinants of health is essential.
I looked for evidence that current efforts were working.
I found one paper, published in 2023 but using data from 2020-2017 (is this even useful?) that suggested RHD Control Programs have contributed to “major success in the management of ARF/RHD through increased delivery of secondary prevention” – despite the fact that Acute Rheumatic Fever (ARF) case numbers were increasing.
The RHD data in the Aboriginal and Torres Strait Islander Health Performance Framework are just as outdated, just as useless.
AIHW data from Queensland, Western Australia, South Australia and the Northern Territory shows that the number and rate of RHD diagnoses among First Nations people increased from a low of 245 (50.9 per 100,000) in 2016 to 299 (54.1 per 100,000) in 2024.
AIHW also reports 2024 data from these jurisdictions on the delivery of secondary prophylaxis (antibiotics to prevent recurrence of ARF. This generally requires injections every 28 days and receiving less than 40 percent of scheduled doses is ineffective; at least 80 percent of doses is considered necessary to provide adequate protection against recurrent ARF.
That’s a tough requirement for healthcare staff and patients to meet in remote communities. And so it is small wonder that in 2024 only 32.4 percent of eligible people received 80 percent or more of their prescribed doses and 33.4 percent received less than 40 percent of their prescribed doses.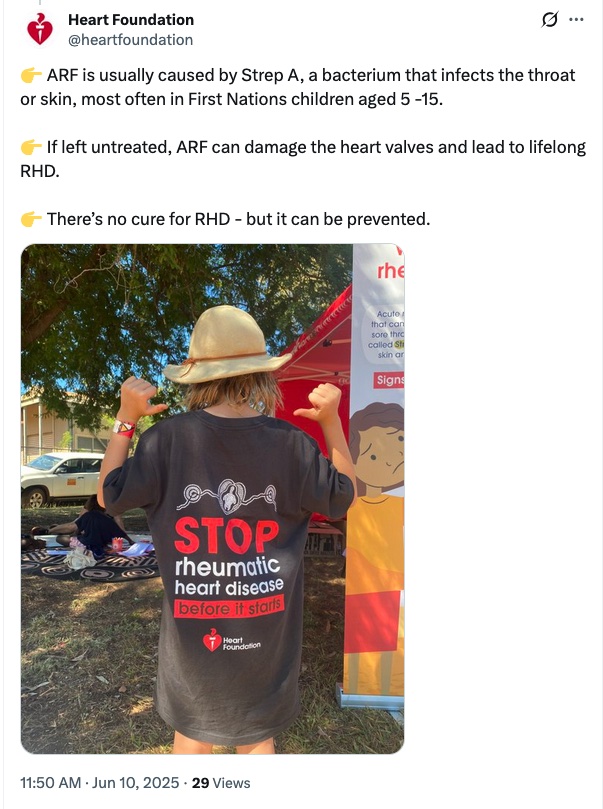
The discussion above makes clear that culturally safe community services make a major difference in the health outcomes for First Nations communities.
The Conversation recently published an article, based on the work of the Indigenous Medication Review Service Feasibility Study (the original paper is here), that highlights how a trusted and safe medication management service delivered by community pharmacists working with Aboriginal and Torres Strait Islander healthcare workers can reduce the incidence of serious medication-related problems and improve consumer health, medication use and wellbeing.
This research on medication management services was designed to address a specific problem: between 16 percent and 74 percent of hospitalisations for Indigenous patients in Queensland for cardiovascular issues, including heart attacks and strokes, were linked to preventable medication problems.
Here’s what the researchers found works:
Allowing patients to choose a safe place for a medicines review, such as the Aboriginal Health Service. Currently, the funding rules require services to be provided at home, which is not preferred by many people
Allowing other trusted care providers – not only GPs – to refer someone for a medication review; these could include Aboriginal Health Workers and nurses
Requiring pharmacists and pharmacy staff to undertake cultural awareness training and use strengths-based motivational interviewing when reviewing medications.
Antarctica’s penguins under threat
Readers may have noticed that after my trip to the Antarctic last year I am paying attention to the impacts of climate change and bird flu on the local wildlife and usually manage to include some new information in each edition of The Health Wrap.
This edition brings more news of dramatic and worrying changes to the penguins’ environment and breeding cycles.
A PBS NewsHour article reports on a study that shows how warming temperatures are forcing Antarctic penguins to breed earlier and that this could mean that several species now face extinction.
Temperatures in the Antarctic breeding grounds increased 5.4 degrees Fahrenheit (3 degrees Celsius) from 2012 to 2022, and this means three different penguin species are beginning their reproductive process earlier.
The study finds that earlier breeding cycles and food preferences mean Adelie and Chinstrap penguins are disadvantaged compared to Gentoos, which are taking over their colony sites. Chinstraps are declining globally and Adelies are doing very poorly in the Antarctic Peninsula. Scientists fear that both species might be extinct before the end of the century.
A paper published in Nature, based on the use of satellite images to assess penguin colonies, finds that Emperor penguins are threatened by the loss of sea ice.
Between 2022 to 2024, reduced fast ice extent resulted in a concentrated distribution of moulting groups and early break-up of the moulting platform before the end of the season. This means the Emperor penguins do not have enough time to regain body condition before they must leave their moulting sites.
It raises a critical question: what is the potential impact of changes in moult habitat on the size of breeding populations in the Ross Sea?
And because Adelie penguins also moult on sea ice, the increasing loss of moulting sites may also affect this species.

This isn’t much to do with public health, social justice, or even the impact of climate change on the habitat of Antarctic penguins, but it is a good news story. I loved watching how the male Gentoo penguins wooed their mates with pebbles for the nest, delivered one-by-one.
So I also loved this story from Edinburgh about how kids in a local hospital paint stones for the penguins at the zoo to use in their wooing ritual.
 https://x.com/washingtonpost/status/2030327937400991803?s=20
https://x.com/washingtonpost/status/2030327937400991803?s=20
Best of Croakey
Over the past three weeks Croakey has done an excellent job of reminding us of the widespread impacts and consequences of the war in the Middle East.
Here’s a list of Croakey articles on these issues that are well worth reading:
As part of Global Public Health Week, Croakey is collaborating with the Medical Association for the Prevention of War in hosting a #CroakeyLIVE webinar to put a focus on peace-making, for health. The event will be from 5-6pm AEST on Wednesday, 8 April.
You can register here.
Good news
I’ve posted about the science competition “Dance your PhD” in previous years; it’s so good I have to do this annually.
The 2026 winners have just been announced here. I particularly like the Social sciences category winner: a young woman from the University of Colorado at Boulder with “The Landscape and Socioecological Drivers of Insect Biodiversity in Cities”.
Croakey thanks and acknowledges Dr Lesley Russell for providing this column as a probono service to our readers. Follow her on Twitter at @LRussellWolpe.
Previous editions of The Health Wrap can be read here.
Readers may also enjoy the Dance your PhD biology category winner: Laura Ihalainen, University of Eastern Finland, “Quantifying the benefits and cost-effectiveness of Real-Ear Measurements (REM) for hearing aid fitting”