

In early 2026, as the United States approached the loss of its measles elimination status—a public health achievement maintained for more than 25 years—Dr. Ralph Abraham, the principal deputy director of the Centers for Disease Control and Prevention (CDC), offered a blunt assessment. Asked whether this reversal mattered, Abraham replied that it was “not really” significant, describing the return of a vaccine-preventable disease as simply the “cost of doing business” in a globalized world.
Abraham further sought to shift responsibility overseas by pointing to “somewhat porous” borders and international travel. Yet this explanation is contradicted by CDC surveillance data. Only a small fraction of measles cases are imported into the United States; the overwhelming majority arise from sustained domestic transmission within under-vaccinated communities. In 2025, more than 2,200 measles cases were confirmed nationwide—the highest annual total since 1992. Outbreaks have been concentrated on vulnerable populations, including a documented spread at the Dilley Immigration Processing Center in South Texas, where detainees are confined in high-risk congregate conditions.
This resurgence is not an accident, nor the product of unavoidable global forces. It is the outcome of a deliberate dismantling of public health infrastructure under Health and Human Services Secretary Robert F. Kennedy Jr. Since taking office, Kennedy has removed scientific experts from advisory roles, dismissed the entire Advisory Committee on Immunization Practices, and undermined the vaccination programs built in the 1960s that sharply reduced childhood illness and death across the United States.
The historical record is clear. Between 2000 and 2015 alone, measles vaccination prevented an estimated 20.3 million deaths worldwide, according to joint WHO–CDC modeling. This was not a marginal gain, but one of the most successful disease-prevention efforts in modern history. Under the current administration’s banner of “health freedom,” that progress is being rapidly reversed. In January 2026 alone, the United States reported 588 measles cases, placing the country on a trajectory to far exceed the already devastating totals of the previous year.
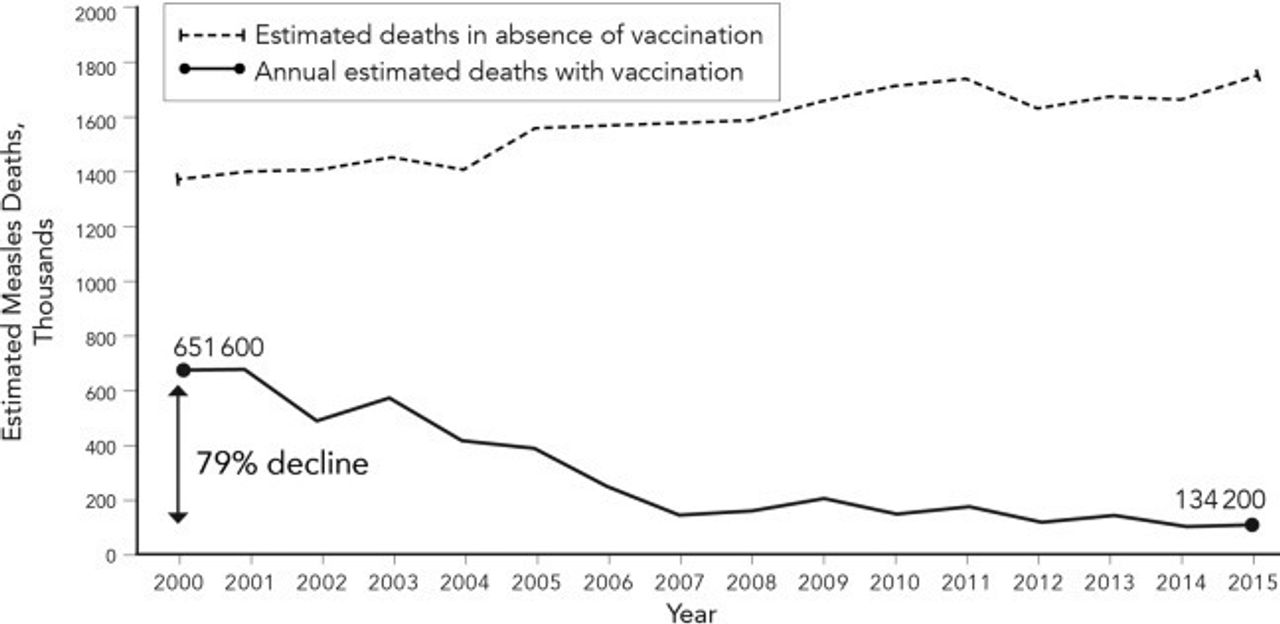 Graph shows lives saved through measles vaccination between 2000 and 2025. [Photo: WHO-CDC]
Graph shows lives saved through measles vaccination between 2000 and 2025. [Photo: WHO-CDC]
Abraham’s fatalism stands in sharp contrast to the scientific ambition that once defined the CDC. Alexander Langmuir, the founder of the Epidemic Intelligence Service and the agency’s first chief epidemiologist, regarded the conquest of disease as a moral obligation. In his 1962 address, “The Importance of Measles as a Health Problem,” Langmuir rejected the idea that society must simply “learn to live” with endemic infection. Instead, he argued for eradication, declaring that measles should be eliminated “because it is there—and because it can be done.”
 Alexander Langmuir
Alexander Langmuir
Langmuir understood that the balance between humanity and disease was not fixed but could be altered through organized scientific action. That outlook has since been abandoned. By elevating officials like Abraham, who is not trained as an epidemiologist, to senior leadership positions, Kennedy has effectively constrained the CDC’s capacity to carry out its central mission: the prevention and control of disease. The shift from Langmuir’s confidence that eradication “can be done” to Abraham’s resignation that illness is merely the “cost of doing business” marks a fundamental transformation of the agency from a defender of public health into an instrument of its erosion.
In order to understand more fully the degree of social and scientific regression represented by the Trump-Kennedy-Abraham “school” of anti-vaccine propaganda, it is necessary to review the protracted historical development of science and public health out of which modern vaccination practices arose.
Edward Jenner and Louis Pasteur
One of the most critical steps in the understanding of viruses and how to combat them was the discovery of attenuation: that viruses passed through nonhuman hosts often lost their ability to cause severe disease in humans while still triggering an immune response which protected against future infection. Cowpox, a relative of smallpox, followed this path as it circulated through animal reservoirs before infecting cattle, becoming far less dangerous to humans in the process.
 Dr. Jenner performing his first vaccination, oil painting by Ernest Board, c. 1912.
Dr. Jenner performing his first vaccination, oil painting by Ernest Board, c. 1912.
In 1796, Edward Jenner, a rural physician in England, translated this observation into practice. He noted that dairymaids who contracted cowpox did not develop smallpox. He then deliberately inoculated an eight-year-old boy, James Phipps, with material taken from a cowpox lesion. When later exposed to smallpox, the child remained healthy. Jenner had no theory of viruses or immunity, but he had demonstrated that exposure to a weakened relative of a deadly pathogen could confer protection. Vaccination, though not yet understood theoretically, had begun in human practice.
Nearly a century passed before this empirical insight was incorporated into science. That shift came with Louis Pasteur, who replaced observation and folklore with controlled experimentation. Trained as a chemist, Pasteur entered biology through his work on fermentation, demonstrating that microbial life, not spontaneous chemical decay, drove biological processes. This insistence on living agents as causal forces laid the foundation for modern microbiology.
Pasteur’s decisive contribution to vaccinology came in 1879 through an accident. Cultures of the bacterium responsible for chicken cholera, left unattended in his laboratory, lost their lethality. When injected into animals, these weakened microbes caused mild illness but conferred protection against subsequent exposure to virulent strains. Pasteur recognized the significance immediately: the virulence was not fixed. It could be reduced, controlled and exploited.
He soon demonstrated this principle publicly. In 1881, at a widely attended field trial at Pouilly-le-Fort, sheep vaccinated with an attenuated anthrax strain survived deliberate exposure to lethal bacteria, while unvaccinated animals died. The result settled scientific debate and established attenuation as a reproducible method rather than a curiosity.
 Louis Pasteur
Louis Pasteur
Pasteur’s final test came with rabies, a disease that inspired widespread fear. Unable to culture the virus directly, he weakened it by passing it through rabbits and drying their spinal cords, reducing virulence with each step. In 1885, when a nine-year-old boy was bitten by a rabid dog, Pasteur administered the experimental treatment. The child survived. For the first time, a fatal infection had been prevented after exposure.
By the end of the 19th century, vaccination had been transformed. What Jenner had discovered by observation, Pasteur had rendered deliberate and systematic. Attenuation was no longer a gift of chance or nature, but a method—one that would later allow scientists to weaken viruses with precision and turn once-inevitable childhood diseases into preventable relics.
Hans Zinsser and John Franklin Enders
By the early 20th century, the center of scientific innovation had begun to shift from the European pioneers of bacteriology to a new generation intent on institutionalizing their breakthroughs. One of the most important figures in this transition was Hans Zinsser, a professor at Harvard Medical School who embodied the passage from nineteenth-century natural history to modern laboratory science. Zinsser was a bacteriologist by training, but also a historian and literary figure, best known for his 1935 book Rats, Lice and History, which treated infectious disease not as a medical curiosity but as a force that shaped civilizations and determined the outcomes of wars.
Zinsser lived at a moment when medicine was rapidly transforming from what he himself described as a “meagerly scientific art” into a disciplined experimental science. Born in 1878 and dying in 1940, his career spanned the final triumphs of Pasteurian bacteriology and the emergence of antibiotics. He belonged to a generation that viewed the conquest of infectious disease as neither accidental nor miraculous, but as a social obligation grounded in reason and method. Disease, to Zinsser, was not merely an object of study, but an adversary in what he called “one of the few genuine adventures left in the world.”
 Hans Zinsser
Hans Zinsser
At Harvard, Zinsser fostered an environment that rejected narrow specialization. His laboratory blurred the boundary between science and the humanities, encouraging students to think historically, philosophically and biologically all at once. Scientific rigor, he argued, was inseparable from intellectual breadth. He described this outlook as a “New Humanism,” a conviction that uncovering order in nature carried moral as well as practical significance.
It was within this setting that John Franklin Enders, a wealthy scion of a prominent Connecticut banking family, found his direction. Introduced to Zinsser’s laboratory through a medical student friend, Enders encountered a form of science that joined disciplined experimentation with clear human purpose. Zinsser presented microbiology not as technical labor, but as meaningful work with direct consequences for human life. Under his influence, Enders abandoned his stalled literary studies into Celtic and Germanic languages and committed himself to laboratory research.
Zinsser’s mentorship was less about technique than temperament. He taught Enders that patience, careful observation and wide intellectual curiosity were as essential to scientific discovery as any instrument or protocol. In this way, Zinsser served as a bridge between the empirical traditions of the 19th century and the technical precision that would define 20th-century virology. That bridge would carry Enders toward the breakthroughs that made the cultivation of poliovirus and the isolation of measles virus possible.
Enders’ financial independence made him an anomaly in academic medicine. After completing his scientific training in 1930, he remained in the Harvard faculty for more than a decade without pressure to publish rapidly or compete for grants. Known to his students simply as “The Chief,” he cultivated a modest, patient style of investigation. He kept portraits of his trainees on his office wall, favored small, focused experiments, and resisted the culture of haste that increasingly dominated biomedical research.
This unhurried approach proved decisive. Through painstaking studies of viruses such as mumps and feline distemper (a highly contagious and often fatal viral disease of cats), Enders developed a deep understanding of viral behavior in tissue culture. That combination of technical rigor, intellectual curiosity and insulation from immediate financial constraint positioned him to challenge the assumptions that had stalled vaccine development. It was under these conditions that Enders would go on to help unlock the cultivation of poliovirus and, soon after, the isolation of the measles virus itself.
Mehring Books
The Wuhan Lab Lie and the Fight for Scientific Truth
This pamphlet provides an overview of the principled stand taken by the WSWS against the far-right Wuhan Lab Lie. It is essential reading for all those seeking to defend science and public health.
Breakthrough in culturing the poliovirus
In 1946, Enders established a new laboratory at Boston Children’s Hospital, bringing together two younger collaborators, Thomas Weller and Frederick Robbins. At the time, the field of virology was stalled by what many researchers regarded as an insurmountable problem: poliomyelitis.
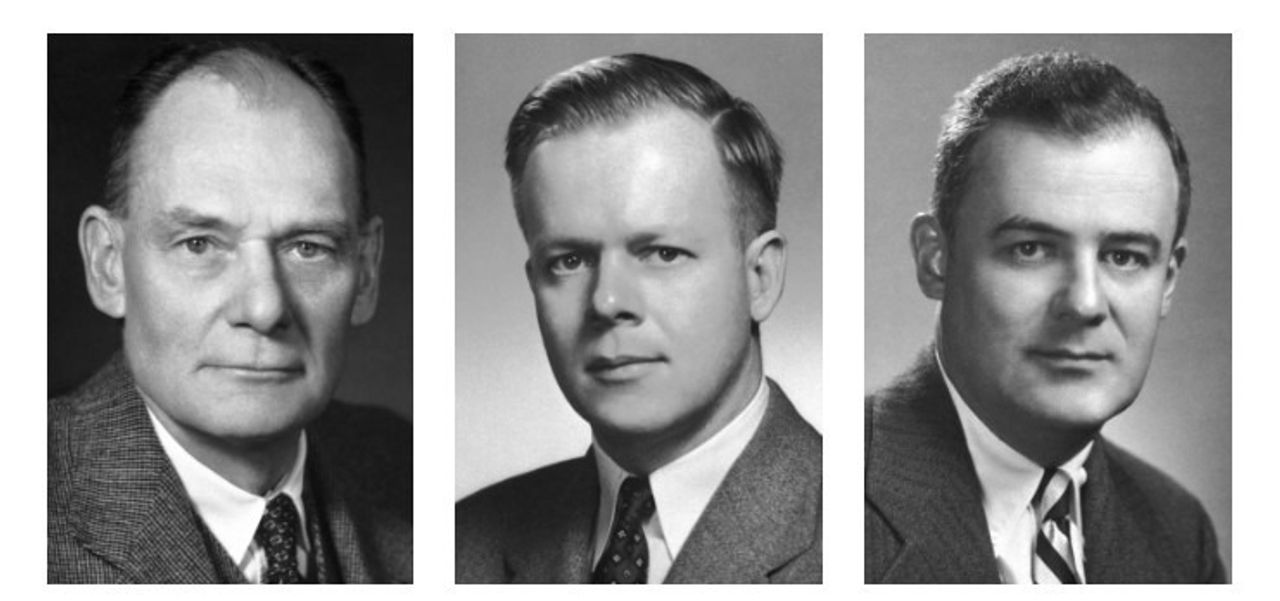 John Franklin Enders, Frederick Robbins, Thomas Weller
John Franklin Enders, Frederick Robbins, Thomas Weller
Prevailing scientific doctrine held that poliovirus was a “strict neurotrope,” capable of replicating only in nerve tissue. This assumption imposed severe practical limits on research. Nervous tissue was difficult to maintain outside the body and dangerous to use in vaccine production, since contamination with neural material risked triggering autoimmune inflammation. As a result, poliovirus was propagated almost exclusively in the brains and spinal cords of live monkeys. The method was costly, ethically troubling and technically inefficient, yielding only small amounts of virus heavily contaminated with neural debris.
The discovery that overturned this impasse came in 1949 and was driven as much by careful method as by circumstance. Enders, Weller and Robbins were not initially attempting to solve the polio problem. Their original aim was to culture varicella, the virus responsible for chickenpox, using human embryonic skin and muscle tissue—cells selected precisely because they were not neural. With the Lansing strain of poliovirus stored nearby, the researchers made the decision to introduce it into these same cultures.
What distinguished this experiment from earlier failures was the use of tools unavailable to previous generations. By incorporating penicillin and streptomycin into their nutrient medium, the team prevented bacterial contamination that had long plagued tissue culture work. Using the roller-tube technique, in which test tubes were slowly rotated to alternately bathe cells in nutrients and air, they created stable conditions that allowed viral growth to proceed uninterrupted.
The outcome was decisive. Under a standard light microscope, the researchers observed what they termed the cytopathic effect. The poliovirus did not merely persist in skin and muscle cells; it destroyed them. Healthy, elongated cells rounded up, became refractile, and disintegrated, leaving clear gaps in the cell layer. For the first time, viral replication could be observed directly in a glass tube, eliminating the need to rely on animal paralysis or death as an experimental endpoint.
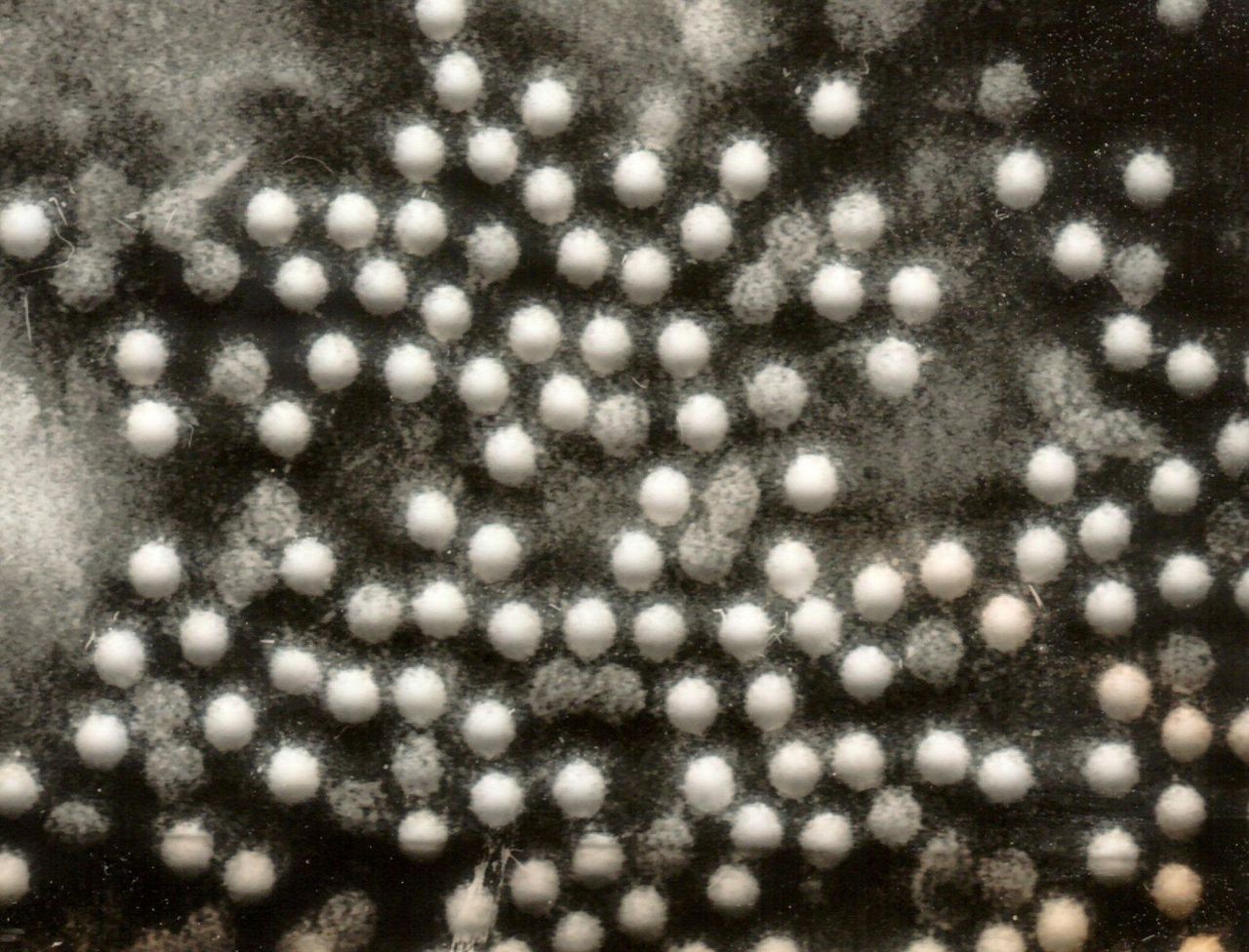 Polio virus under the microscope
Polio virus under the microscope
This discovery, published in Science in 1949, transformed the field. It earned Enders, Weller and Robbins the 1954 Nobel Prize in Physiology or Medicine and provided the practical foundation for modern polio vaccines. Jonas Salk could now grow large quantities of viruses in tissue culture for chemical inactivation, while Albert Sabin could use the same system to select and weaken live viral strains. Consistent with his role as a mentor rather than a rival, Enders declined to accept the Nobel Prize unless it was shared equally with Weller and Robbins, an uncommon gesture in the competitive hierarchy of biomedical research.
Culturing the measles virus and the first vaccine
With the problem of culturing poliovirus solved, Enders turned his attention to measles. By the early 1950s, measles was widely regarded by the public as an unavoidable rite of childhood, even as statisticians recognized it as a major cause of death, claiming millions of lives worldwide each year. Although the viral nature of measles had been demonstrated as early as 1911, the virus had resisted consistent laboratory cultivation for more than four decades. Researchers could transmit the disease to monkeys, but they could not sustain the virus in vitro long enough to study it systematically or develop a vaccine.
The breakthrough came during a localized outbreak in 1954. When measles swept through Fay School, a private boarding school for boys in Southborough, Massachusetts, Enders sent his research fellow Thomas Peebles to investigate. A Harvard-trained physician, Peebles approached the task as a mission. As he collected throat swabs and blood samples from sick students, he reportedly told one boy, “Young man, you are standing on the frontiers of science.”
Back at Boston Children’s Hospital, Peebles inoculated the samples into a rare and carefully maintained supply of human kidney cells. These cultures were obtained from a pediatric neurosurgeon who removed small amounts of healthy kidney tissue during operations to treat hydrocephalus. For weeks, nothing appeared to happen. Then one culture, which was derived from the blood of an 11-year-old student named David Edmonston, began to change. Under the microscope, the normally uniform sheet of cells fused into large, multinucleated structures with a hollowed, “Swiss cheese” appearance. This phenomenon, known as syncytium formation, had a distinctive cytopathic effect. The measles virus had finally been isolated.
Isolation alone, however, was not enough. To transform a wild, disease-causing virus into a usable vaccine, Enders relied on the established technique of serial passage. The principle was simple but exacting: force the virus to adapt to unfamiliar environments until it lost its ability to cause serious disease in humans while retaining its capacity to provoke immunity.
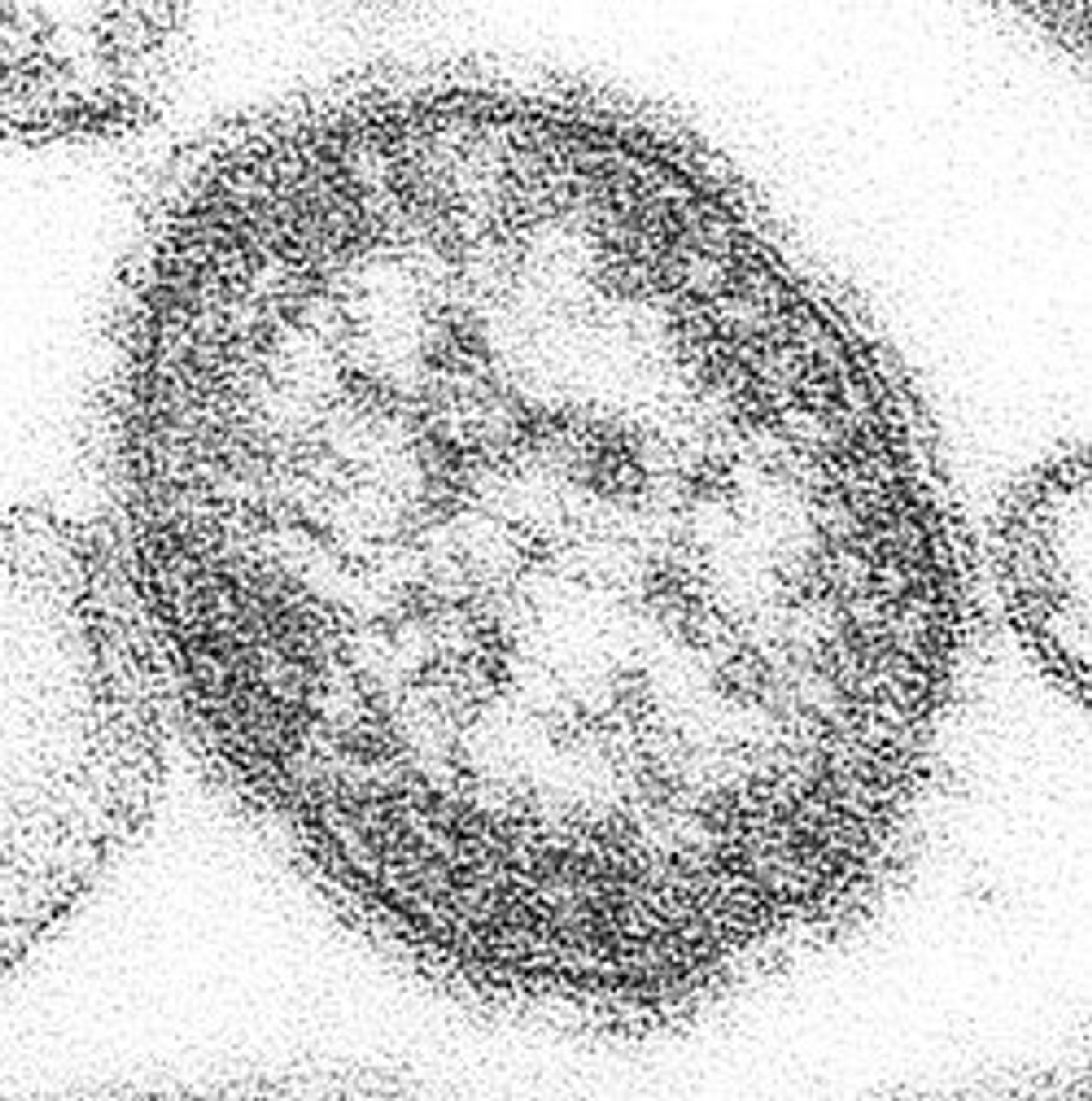 A measles virion (single particle of virus) seen through an electron microscope
A measles virion (single particle of virus) seen through an electron microscope
The Edmonston strain was first stabilized in human kidney cells, allowing it to replicate reliably in the laboratory. It was then transferred to human amnion (thin inner membrane of the placenta that surrounds and protects the fetus during pregnancy) cells, where subtle but important changes appeared. Under the microscope, the virus no longer produced dense clusters of fused cells, but instead formed thin, irregular, star-like patterns, a sign that it was mutating and altering its behavior. The next step forced the virus across a major biological barrier by introducing it into fertilized chicken eggs. Most viral particles failed to adapt and died. A small number, however, acquired mutations that allowed them to enter and replicate in avian cells, even though these cells lacked the receptors normally used by wild-type measles virus in humans.
Those surviving variants were then passed repeatedly through chick embryo cells. With each passage, the virus became better adapted to its new environment and less effective at replicating in human tissue. By the end of this process, the virus had been attenuated. It could still stimulate the immune system, but it no longer caused full-blown disease.
The resulting strain, known as Edmonston-B, accumulated dozens of mutations and replicated efficiently in chicken cells while remaining weakened in human hosts. When Samuel Katz, another member of Enders’ group, tested the vaccine on himself and laboratory colleagues, it proved safe. Field trials soon followed at the Walter E. Fernald State School, an institution that had suffered repeated and deadly measles outbreaks. The vaccine successfully interrupted transmission and demonstrated strong protective effects.
Despite its effectiveness, Edmonston-B was not yet ideal. Many vaccinated children developed high fevers and rashes, often requiring simultaneous administration of gamma globulin to blunt the reaction.
Maurice Hilleman and the “Moraten” strain of the measles vaccine
The task of converting this laboratory success into a usable public health tool fell to Maurice Hilleman, head of virus and vaccine research at Merck & Co. Hilleman stood in marked contrast to Enders. Raised on a Montana farm during the 1919 influenza pandemic and orphaned shortly after birth, he was blunt, impatient with abstraction, and focused almost entirely on outcomes. Where Enders sought understanding, Hilleman sought production. As he later put it, “I came off a farm. I wanted to make things.”
When Hilleman received the Edmonston strain in 1961, he quickly identified a critical problem overlooked in the academic setting. The virus stock was contaminated with avian leukosis virus, a chicken leukemia virus commonly present in embryonated eggs used for viral culture. Drawing on his familiarity with agricultural disease, Hilleman traced the source to infected poultry flocks and located a specific ALV-free flock in California. By rebuilding the vaccine stock from clean material, he established safety controls that would later become standard across vaccine manufacturing.
Hilleman then focused on reducing the virus’s remaining virulence. He subjected the Edmonston strain to roughly 40 additional passages in chick embryo cells and introduced selection for temperature sensitivity. By growing the virus at approximately 32°C—well below normal human body temperature—he favored mutations that allowed replication in cooler conditions while impairing viral efficiency in human hosts.
 Maurice Hilleman (left), at work with a colleague
Maurice Hilleman (left), at work with a colleague
The result was the Moraten strain, shorthand for “More Attenuated Enders.” Licensed in 1968, it retained strong immunogenicity while eliminating the high fever rates associated with Edmonston-B. The need for accompanying gamma globulin was eliminated, making routine childhood immunization feasible at scale. More than half a century later, the Moraten strain remains the measles vaccine used in the United States, a durable product of Hilleman’s methodical refinement.
From the measles vaccine to MMR
Hilleman’s ability to turn biological contingency into reliable public health tools was demonstrated most clearly in the development of the mumps vaccine. As with Peebles collecting samples during the measles outbreak at the Fay School, Hilleman recognized that scientific opportunity often emerged from immediate human circumstances.

In the early morning hours of March 21, 1963, Hilleman was awakened by his five-year-old daughter, Jeryl Lynn, who complained of a sore throat and a swollen jaw—classic signs of mumps, then a near-universal childhood infection and a leading cause of acquired deafness. Rather than treat the illness as inevitable, Hilleman acted. He drove to his laboratory to retrieve culture materials, returned home to collect a throat sample, and preserved the virus for study.
Using techniques refined during his work on measles, Hilleman attenuated the virus through serial passage in chick embryo cells. By 1967, the resulting Jeryl Lynn strain was licensed as the first effective mumps vaccine. Its safety was demonstrated early, including through administration to Hilleman’s younger daughter, Kirsten. The vaccine rapidly reduced mumps incidence and its long-term complications, transforming a routine childhood affliction into a preventable disease.
 A key moment in vaccine development, as Maurice Hilleman inoculates his younger daughter Kirsten (center) with a mumps vaccine made from his older daughter Jeryl Lynn (left).
A key moment in vaccine development, as Maurice Hilleman inoculates his younger daughter Kirsten (center) with a mumps vaccine made from his older daughter Jeryl Lynn (left).
Hilleman’s most consequential contribution, however, lay not in any single vaccine but in the consolidation of multiple advances into a coherent immunization strategy. In 1971, he combined the Moraten measles strain, the Jeryl Lynn mumps strain and a rubella vaccine into a single formulation: the MMR. At the time, many researchers feared that combining live attenuated viruses would reduce efficacy or increase adverse reactions. In practice, the opposite proved true.
The MMR vaccine simplified the childhood immunization schedule, replacing six separate injections with two. This reduction in complexity lowered costs, improved compliance and made population-wide disease control feasible. It marked a decisive shift from laboratory success to operational public health at scale.
Prior to the work of Enders and Hilleman, only a handful of vaccines were widely available, and childhood carried a constant risk of infection, disability and death. Today, largely because of these efforts, diseases that once killed millions each year have been pushed to the margins in countries that maintain robust vaccination programs.
Anthony Fauci, former director of the National Institute of Allergy and Infectious Diseases, paid tribute to Hilleman’s central role in this process in an interview with The New York Times, saying, “One person did that.”
This is, of course, an overstatement, since scientific and technical advances are invariably the result of the cumulative work of an array of scientists, and the material progress of society as a whole. But in the course of Hilleman’s career, he developed or substantially improved more than 40 vaccines, including nine of those routinely recommended for children in the United States.
Public health in the postwar boom
The surge in vaccine development associated with figures such as Enders and Hilleman did not arise in isolation. It unfolded within a specific postwar alignment of scientific ambition, state capacity and geopolitical pressure. The expansion of public health infrastructure after World War II was closely bound to the strategic priorities of the United States as it sought to stabilize capitalist societies in the face of economic devastation caused by world war, and the growing influence of socialism.
In the immediate aftermath of the war, much of Europe lay in ruins, while the Soviet Union emerged with immense political prestige following its decisive role in the defeat of fascism. The prospect of social upheaval was widely viewed by Western elites as an existential threat. In this context, improving public health became part of the class strategy of the ruling elite, to make limited concessions to the working class to stave off social revolution. Institutions such as the Centers for Disease Control and Prevention, established in 1946, and the World Health Organization, founded in 1948, were part of a broader effort to reconstruct economies, stabilize labor forces and contain social unrest.
The Marshall Plan, launched in 1948, formed the economic core of this strategy. Publicly presented as a program of reconstruction and aid, it also aimed to rebuild European markets capable of absorbing American industrial output and to counter the appeal of socialist movements. Public health infrastructure played an important role in this project. A population weakened by endemic disease could neither rebuild war-damaged economies nor sustain industrial production. Investment in disease control, including mass vaccination campaigns, functioned as a stabilizing measure within a broader political economy.
The scientists who led the conquest of infectious diseases worked within this environment. Enders, Hilleman and their contemporaries lived through an era marked by revolution, depression and global war, alongside the political struggles associated with figures such as Lenin and Trotsky. Yet they operated largely within insulated institutional settings, including elite universities and well-funded research hospitals, at a time when capitalism could still accommodate reforms such as expansion of public health services.
Many of these scientists understood their work as separate from politics. They approached disease as a technical and biological problem, believing that scientific progress, supported by public institutions, could steadily reduce human suffering. The CDC and WHO appeared to embody this promise: technocratic agencies capable of translating scientific knowledge into global health gains without confronting deeper social antagonisms.
The origins of the CDC underscore this dual character. The agency emerged from wartime necessity, beginning in 1942 as the Malaria Control in War Areas program, designed to protect military installations and industrial production in the southern United States. Its later evolution into a national and international public health authority reflected both scientific advances and the geopolitical requirements of a global power managing disease as a factor of economic and military readiness.
This architecture also enabled limited forms of international cooperation. The eradication of smallpox, initiated by a Soviet proposal to the WHO in 1958 and carried out through coordinated global vaccination, stands as the most notable example. Yet such cooperation remained constrained by the nation-state system and dependent on a temporary alignment of interests between rival powers.
What emerged in the postwar decades was not a permanent settlement, but a historically specific configuration. The expansion of public health rested on economic growth, strong state capacity and the existence of a geopolitical counterweight that compelled concessions to social welfare. Scientists and institutions operated as if this arrangement were stable and enduring. Its fragility would become apparent only later, as the conditions that sustained it began to erode.
The capitalist crisis and the assault on science and public health
The unraveling of this public health consensus did not begin with the COVID pandemic, but with the collapse of the economic order that sustained it. By the late 1960s, the economic supremacy of the United States was eroding, and the costs of the Vietnam War and domestic social programs were increasingly seen as incompatible with profitability. On August 15, 1971, President Richard Nixon suspended the convertibility of the dollar into gold, effectively ending the Bretton Woods system of fixed currencies tied to the dollar. This shattered the foundations of national economic regulation and inaugurated an era of floating exchange rates, the removal of capital controls and the explosive growth of global financial markets operating beyond the control of any single nation-state.
This shift had profound consequences for public health. As production globalized, transnational corporations became increasingly detached from the health and stability of any particular national workforce. The ruling class no longer faced the same material imperative to sustain the social infrastructure—hospitals, surveillance systems and vaccination programs—that had previously underpinned economic and political stability.
With the fading of the postwar boom and the eventual collapse of the Soviet Union, the foundations of this public health architecture began to buckle. The belief that science could operate independently of political economy was exposed as an illusion. The globalization of production and the financialization of the economy came into direct conflict with the nationally based reforms of the postwar period.
This retreat was reflected in a decisive shift in public health strategy. The expansive “Health for All” vision articulated at the 1978 Alma Ata Conference gave way in the 1980s to “selective primary health care,” a model that narrowed public health to discrete, cost-effective, and disease-specific interventions, prioritizing short-term metrics and budgetary efficiency over universal prevention and population-wide protection. Public health was stripped of its broader social mission and reshaped to fit the constraints of neoliberal austerity. The contradictions of the capitalist order, long ignored by the scientific elite, were now bearing down on the very institutions they had helped build.
The accelerating collapse of public health in the seventh year of the COVID-19 pandemic, alongside the resurgence of measles, is not simply a policy failure. It is a symptom of the historical exhaustion of the nation-state system itself. The pandemic functioned as what David North has described as a “trigger event” in world history—an upheaval that exposed the economic, political, social and moral bankruptcy of the capitalist order. Like the outbreak of World War I in 1914, COVID-19 did not emerge from nowhere; it revealed and further intensified contradictions that had been accumulating for decades, shattering the illusion that the nation-state, subordinated to global finance, retains neither the capacity or the will to protect human life.
 Patients wear personal protective equipment while maintaining social distancing as they wait in line for a COVID-19 test at Elmhurst Hospital Center, Wednesday, March 25, 2020, in New York. (AP Photo/John Minchillo)
Patients wear personal protective equipment while maintaining social distancing as they wait in line for a COVID-19 test at Elmhurst Hospital Center, Wednesday, March 25, 2020, in New York. (AP Photo/John Minchillo)
The rise of anti-science and anti-vaccine sentiment, now embedded within state policy, is not an aberration or a temporary fluctuation in public opinion—which remains overwhelmingly in favor of public health efforts. It is an expression of the social and moral decay of the ruling class, which now embraces every form of backwardness and reaction. Having abandoned the limited postwar compromise that once made institutions such as the CDC and the World Health Organization possible, the ruling class can no longer tolerate the allocation of resources to universal disease prevention. Science itself has become an obstacle where it conflicts with profit and militarism.
The pandemic established a principle that has since hardened into state doctrine: profit extraction must be preserved, regardless of the human cost. The normalization of mass death from COVID-19 laid the groundwork for the revival of measles, polio and other preventable diseases. The formal withdrawal of the United States from the WHO in January 2026—leaving the organization on the brink of financial collapse—marked a decisive break with even the limited framework of international health cooperation that had existed since the postwar period. The result is a world increasingly vulnerable to the return of plagues once brought under control.
It would be a mistake to reduce this regression to the actions of individual figures such as Donald Trump or Robert F. Kennedy Jr. They are not the cause, but the expression, of a system in terminal decline. A social order that requires the suppression of science and the sacrifice of the vulnerable to sustain itself has exhausted its historical justification. The regression from Alexander Langmuir’s confidence in 1962 that measles eradication could be achieved “because it is there—and because it can be done,” to Ralph Abraham’s blunt declaration in 2026 that disease is merely the “cost of doing business,” traces the trajectory of a dying system. Barbarism is not a future danger; it has become policy.
For scientists and medical professionals, the implications are unavoidable. The defense of science cannot be separated from the struggle to transform the social order that governs it. The conquest of disease for the benefit of humanity is incompatible with a system organized around private profit and national division. If science is to serve life rather than destruction, those who practice it must align themselves with the only social force whose interests lie in the preservation of human existence: the international working class. The struggle against the microbe has become inseparable from the struggle against capitalism itself.