
Literature search
The initial search across five major databases resulted in 2,485 research articles. After eliminating 578 duplicate entries identified across the databases, a total of 1,907 records were retained for further screening. A screening of titles and abstracts led to the selection of 108 articles for full-text review. Of these, 87 were excluded for various reasons: 22 were excluded due to inappropriate study design, 19 focused on psychiatric disorders other than anxiety, 13 examined non-cardiovascular medications, and 12 lacked a clear definition of medication adherence. An additional 11 studies focused on adherence unrelated to medication, seven were not published in English, two involved paediatric populations, and one was an intervention-based study. Ultimately, 23 studies met all eligibility criteria and were included in the final analysis (Fig. 1). The PRISMA checklist is included as Supplementary file 2.
Fig. 1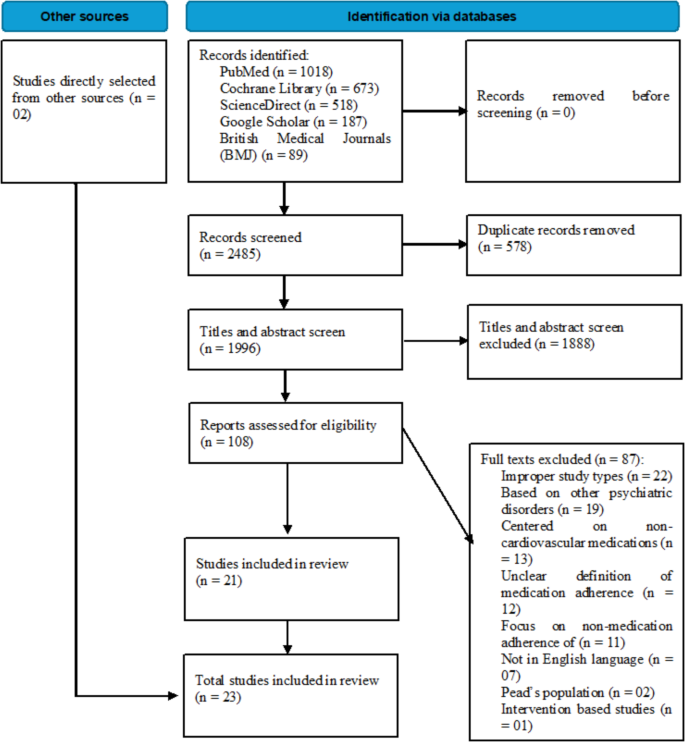
PRISMA flowchart of the searching and screening studies
Quality assessment of included studies
Based on the NIH quality assessment tool, the included studies demonstrated an overall satisfactory level of methodological quality. However, several recurring methodological limitations were identified. For instance, only one study [45] reported blinded outcome assessment, highlighting the risk of detection bias. In 17 studies, sample size justification, while in 18 studies the adequacy of the timeframe to observe outcomes was not addressed. Additionally, 19 studies lacked repeated exposure assessments, limiting the ability to track changes over time. In 18 studies, the follow-up rate was marked “not applicable,” primarily due to their cross-sectional design. Despite these issues, majority of studies met the remaining nine of the 14 NIH criteria. A detailed summary of quality scores is shown in Table 1.
Table 1 Quality Evaluation of Included Studies Using the National Institutes of Health (NIH) Tool for Observational Cohort and Cross-Sectional Studies [43], [1,2,3, 8, 12, 13, 16,17,18,19,20, 23, 25, 28, 34,35,36,37, 45, 50, 52, 55, 56]Baseline characteristics
Among the included studies, 18 employed cross-sectional design, while 5 utilized a longitudinal approach. Geographically, the studies were conducted across various global regions, including Asia (n = 9), Europe (n = 8), North America (n = 3), Africa (n = 2), and Australia (n = 1).
The cumulative sample size across all studies was 72,815 participants. The largest sample was reported by Kim et al. comprising 57,105 individuals (H. K. [34]), while six studies included more than 1,000 participants, thereby enhancing the statistical power of their findings. In contrast, the smallest sample was noted in the study by Sudana and Asih (2019), which included 55 participants (Sudana & Asih, 2019). The mean age of participants, as reported in 15 studies, was 60.7 years. The average proportion of male participants, based on data from 22 studies, was 51.7%. Reported study durations ranged from 6 months to five years.
Among the drug classes, antihypertensive medications were the most frequently studied (n = 8), followed by medications for CHF, IHD, and other CV conditions each examined in five studies. Anxiety was most frequently assessed using the Hospital Anxiety and Depression Scale-Anxiety subscale (HADS-A), which was utilized in nine studies. Similarly, definitions of medication adherence varied, with six studies using the Morisky Medication Adherence Scale (MMAS), and four using a ≥ 80% threshold of days covered. Baseline characteristics of the included studies are detailed in Table 2.
Table 2 Summary of the included studies examining the relationship between anxiety disorders and medication adherence in patients with cardiovascular diseasesImpact of anxiety on medication adherence
The included studies revealed three overarching patterns concerning the association between anxiety disorders and adherence to CV medications.
Majority of studies (n = 15), comprising 11 cross-sectional (n = 9,103) [1, 2, 8, 13, 17,18,19, 25, 28, 35, 56] and four longitudinal investigations (n = 3,283) [3, 20, 23, 36], reported a negative relationship, whereby elevated anxiety levels were associated with reduced medication adherence. While cross-sectional studies identified this relationship at a single time point, the longitudinal studies offered more robust evidence, demonstrating that both baseline anxiety and increases in anxiety symptoms over time were predictive of poorer adherence outcomes. This negative association was consistently observed across clinical subgroups, with supporting findings reported in 5 of 8 hypertension studies, 2 of 5 studies on CHF, 4 of 5 studies on IHD, and 4 of 5 studies addressing other CV conditions. There were three studies (n = 6,029) [8, 17, 23] reported their findings based on a combined assessment of anxiety and depression. As a result, the observed associations in these studies may be confounded by the overlapping effects of both these conditions.
Among the 15 studies, three studies examined gender as a moderator of the negative anxiety–adherence relationship. In Korhonen et al., women with frequent anxiety symptoms demonstrated a higher relative risk of nonadherence (RR = 1.38) compared to men (RR = 1.24); however, this interaction was not statistically significant (p = 0.38) [36]. In contrast, Gentil et al. found a significant gender interaction, where men with anxiety or depressive disorders had significantly higher odds of nonadherence (AOR = 2.39) then women (AOR = 0.92) [23]. Supporting this gender-related trend, Eisele et al. also reported that male sex, along with higher educational level, was independently associated with reduced adherence (odds ratio < 1) [17].
A subset of five studies (n = 2,289)—four cross-sectional and one longitudinal—found no significant association between anxiety and adherence. Among these, two studies were focused on CHF [45, 50], and one each on hypertension [37], IHD (Sudana & Asih, 2019), and mixed CV conditions [55]. Notably, the longitudinal study by Rasmussen et al., which followed 1,464 CHF patients over a three-year period, concluded that anxiety was not a significant predictor of non-adherence. Similar conclusions were reported in the four cross-sectional studies, which also found no independent link between anxiety and adherence. However, similar to the three studies reporting a negative association, one study (n = 255) [55] also presented its findings based on a combined measure of anxiety and depression.
There were three cross-sectional studies, encompassing 58,140 participants, which reported that individuals with anxiety were more likely to adhere to their CV medications. In particular, Kim et al. using data from a large Korean cohort of 57,105 individuals with hypertension, observed slightly higher adherence rates among those with anxiety disorders (Ha Kyoung [34]). This finding was echoed in Deek and Massouh, who reported a similar association in hypertensive patients [12], and in Dyussenova et al., who found that CHF patients with elevated anxiety levels demonstrated greater adherence [16].
Meta-analysis
A total of 20 studies were included in the meta-analysis investigating the relationship between anxiety and medication adherence among patients with CV diseases. The pooled SMD = −1.087, 95% CI [−1.469, −0.705], p < 0.001, indicating a statistically significant negative association, whereby higher anxiety levels were associated with lower medication adherence (Fig. 2). The analysis revealed substantial heterogeneity across studies (I2 = 99.38%), suggesting considerable variability in effect estimates. Although the funnel plot indicated slight asymmetry, with a greater number of studies showing negative effect sizes, Egger’s regression test did not detect significant publication bias (p = 0.160) (Fig. 3).
Fig. 2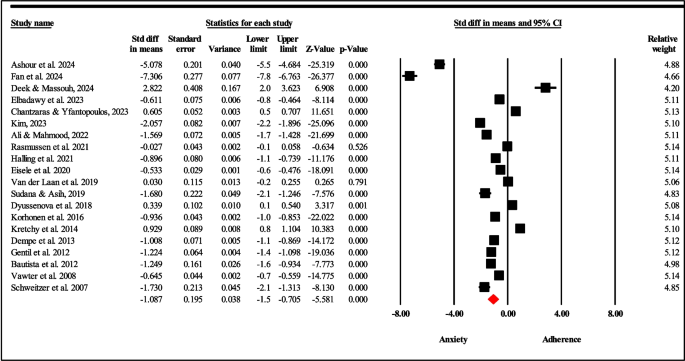
Forest plot of studies on anxiety and medication adherence in cardiovascular (CV) disease
Fig. 3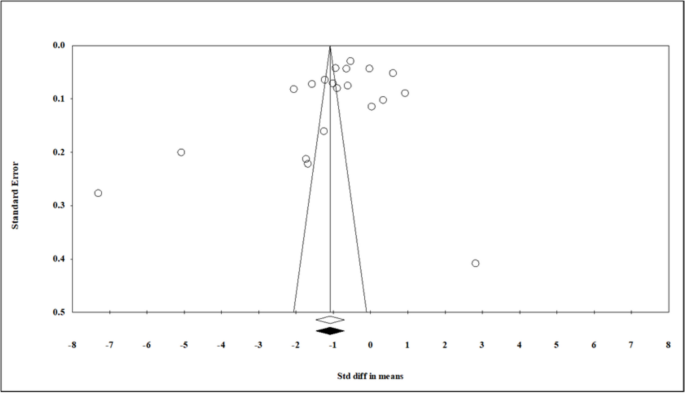
Funnel plot of studies on anxiety and medication adherence in cardiovascular (CV) disease
The sensitivity analysis (n = 18) demonstrated that the exclusion of two studies with extreme effect sizes [2, 19] had a modest influence on the pooled effect. Nonetheless, the overall effect remained statistically significant (SMD = −0.561, 95% CI [−0.9, −0.237], p = 0.001).
Subgroup analysisSubgroup Analysis by Cardiovascular (CV) Disease Type
In the subgroup analysis based on CV type, three categories were assessed. The HTN subgroup, which included seven studies yielded a pooled SMD = −0.648, 95% CI [−1.293, −0.004], p = 0.049, indicating a statistically negative significant association between anxiety and medication adherence in this population. The studies exhibited a high level of heterogeneity (I2 = 99.46%), showing considerable variation in the reported outcomes. In case of CHF subgroup (n = 4), the pooled SMD = −0.51, 95% CI [−0.92, −0.10], p = 0.02, indicating a statistically significant negative association between anxiety and medication adherence. Nonetheless, heterogeneity among the included studies was high (I2 = 97.99%). Similarly, for the IHD subgroup (n = 4), the pooled SMD = −2.322, 95% CI [−3.498, −1.146], p < 0.001), reflecting a strong and statistically significant inverse relationship. This analysis also revealed high heterogeneity among studies (I2 = 99.18%).
Subgroup analysis by anxiety and adherence measurement tools
In the second category of subgroup analysis, stratification was performed based on the tools used to assess anxiety and medication adherence. Among studies employing the HADS-A scale, the pooled SMD = −2.008, 95% CI [−2.752, −1.265], p < 0.001), indicating a statistically significant negative association, although heterogeneity was high (I2 = 99.18%). With regard to adherence assessment tools, two subgroup analyses were conducted. For studies utilizing the MMAS, the pooled effect size also suggested a negative association, though the result was not statistically significant (SMD = −0.412, 95% CI [−0.933, 0.109], p = 0.121), with high heterogeneity (I2 = 98.75%). Similarly, studies defining adherence using the 80% days covered threshold yielded a negative but non-significant association (SMD = −0.539, 95% CI [−1.148, 0.069], p = 0.083), also marked by high heterogeneity (I2 = 98.75%).
Subgroup analysis by geographic region
A subgroup analysis was performed according to geographic region, separating studies conducted in Asia and Europe. Among the studies from Asian countries, the pooled results indicated a statistically significant inverse relationship between anxiety and medication adherence (SMD = −2.090, 95% CI [−3.463, −0.717], p = 0.003), though heterogeneity was high (I2 = 99.51%). In contrast, studies conducted in European countries also showed a negative association, but it did not reach statistical significance (SMD = −0.396, 95% CI [−0.817, 0.026], p = 0.066), and heterogeneity remained substantial (I2 = 99.20%). The supplementary figures and statistical details of the meta-analysis are included in supplementary file 3.