
Breadcrumb Trail Links
Acute care beds per 1,000 people has fallen from 2.05 in 2017 to 1.59 last year. Our weekly Countdown to 2 Million special series continues.
Published Mar 04, 2026 • Last updated 1 hour ago • 18 minute read
You can save this article by registering for free here. Or sign-in if you have an account.
 The Foothills Hospital was photographed on Wednesday, May 19, 2021. Photo by Gavin Young/PostmediaArticle content
The Foothills Hospital was photographed on Wednesday, May 19, 2021. Photo by Gavin Young/PostmediaArticle content
Fahima Mustanzid yearns to play a bigger role in finding a health-care solution in the fast-growing city she’s called home after leaving Bangladesh in 2013.
But as an international physician, she said it’s been a long, frustrating road to acquiring the qualifications needed to fulfil her dream of practising psychiatric or family medicine in Calgary.
Article content
Article content
She’s twice travelled back to her native Bangladesh to work in that country’s health-care system to attain those credentials but balked, due to the difficulties in raising two young sons, when told a third trip was required.
Advertisement 2
This advertisement has not loaded yet, but your article continues below.
![]()
THIS CONTENT IS RESERVED FOR SUBSCRIBERS ONLY
Subscribe now to read the latest news in your city and across Canada.
Unlimited online access to articles from across Canada with one account.Get exclusive access to the Calgary Herald ePaper, an electronic replica of the print edition that you can share, download and comment on.Enjoy insights and behind-the-scenes analysis from our award-winning journalists.Support local journalists and the next generation of journalists.Daily puzzles including the New York Times Crossword.
SUBSCRIBE TO UNLOCK MORE ARTICLES
Subscribe now to read the latest news in your city and across Canada.
Unlimited online access to articles from across Canada with one account.Get exclusive access to the Calgary Herald ePaper, an electronic replica of the print edition that you can share, download and comment on.Enjoy insights and behind-the-scenes analysis from our award-winning journalists.Support local journalists and the next generation of journalists.Daily puzzles including the New York Times Crossword.
REGISTER / SIGN IN TO UNLOCK MORE ARTICLES
Create an account or sign in to continue with your reading experience.
Access articles from across Canada with one account.Share your thoughts and join the conversation in the comments.Enjoy additional articles per month.Get email updates from your favourite authors.
THIS ARTICLE IS FREE TO READ REGISTER TO UNLOCK.
Create an account or sign in to continue with your reading experience.
Access articles from across Canada with one accountShare your thoughts and join the conversation in the commentsEnjoy additional articles per monthGet email updates from your favourite authorsSign In or Create an Account
or
Article content
“The rules keep changing. They change very fast,” said Mustanzid, 38.
![]()
Noon News Roundup
Thanks for signing up!
Article content
But Mustanzid refuses to give up, throwing herself into new studies and exams toward gaining a medical residency in Calgary before realizing a full practise.
Interim work as a clinic assistant or manager in Calgary has illustrated just how much more physicians, including eager-to-work international doctors, are needed.
“I’ve seen the huge suffering of patients at the clinic, seeing people who couldn’t get into emergency — it’s very frustrating how people are struggling,” said Mustanzid.
“We’re a big resource Canada could benefit from.”
 International physician Fahima Mustanzid was photographed at the Alberta International Medical Graduates Association (AIMGA) offices in Calgary on Wednesday, February 25, 2026. Photo by Gavin Young/Postmedia
International physician Fahima Mustanzid was photographed at the Alberta International Medical Graduates Association (AIMGA) offices in Calgary on Wednesday, February 25, 2026. Photo by Gavin Young/Postmedia
She’s already been an advocate for renewing the province’s approach to mental health care that she believes could benefit from international physicians’ fresh perspective.
“Canada is my home and I have to look for gaps that can be improved,” said Mustanzid.
According to Alberta Health Services, the hiring of psychiatric physicians is expected to be greater than all other medical sectors, with 10-year growth pegged at 47 per cent higher than current levels.
The province’s complement of international physicians struggling for qualification is oversized — 1,200 out of the 3,700 across the country — and represent a significant pool of talent, says Deidre Lake, executive director of the Alberta International Medical Graduates Association.
“Some barriers are being removed but in some places, barriers are being put in place to make it more difficult,” she said.
Article content
Mustanzid realizing her goal would add one piece to a complex aspirational puzzle assembled to meet the health care demands of a rapidly-growing city headed to a population of 2 million sometime in the next decade.
But according to some who’ve worked within and observed the evolution of Alberta’s health care system, it’s been a story of regression and attempts to merely keep pace with the present.
“We’re playing catch-up,” said Dr. Raj Sherman, an Edmonton-area emergency room physician who served as Alberta’s associate health minister from 2008 to 2010.
The province has been making up some of the ground lost during the 1990s when the Progressive Conservative government of then-premier Ralph Klein slashed health-care spending and reduced the number of nurses and doctors by 20 per cent in a bid to balance the province’s budget, he said.
In Calgary, the Grace and Holy Cross Hospitals were closed and the Calgary General Hospital in Bridgeland explosively demolished. In 2012, some of that loss was recouped with the opening of the Calgary South Health Campus.
“That’s when health care got broken — other provinces have had challenges but Alberta did it the worst,” said Sherman, a former Liberal MLA.
“We have staff for four million people with a (provincial) population of five million.”
The number of acute care beds in Alberta that stood at 11,700 in the early 1990s now sits at 8,800, while the population has nearly doubled.
Article content
That’s seen the bed-per-patient ratio in the province plummet from 4.3 beds per thousand people to 2.4 beds, said Sherman, who once chaired the Health Quality Council of Alberta but quit in frustration over the level of spending in the system.
Calgary, a city which had 3,000 acute care beds in 1994 now counts 2,703, which includes the Alberta Children’s Hospital even though the population has more than doubled since then. Acute care beds per 1,000 people has fallen from 2.05 in 2017 to 1.59 last year.
“Calgary’s system is stressed like the rest of Canada and maybe more because of the growth,” said Sherman, adding the city and province are in the perfect medical storm.
“We’re five million people now and we’re older and sicker — we’re victims of our own economic success where you now have people with heart diseases live long enough to get cancer.”
 UCP Edmonton-Whitemud candidate Dr. Raj Sherman takes part in a press conference where Danielle Smith announced the UCP’s public health guarantee, in Sherwood Park Tuesday April 11, 2023. Photo by David Bloom
UCP Edmonton-Whitemud candidate Dr. Raj Sherman takes part in a press conference where Danielle Smith announced the UCP’s public health guarantee, in Sherwood Park Tuesday April 11, 2023. Photo by David Bloom
He cites a Danish model of medicine that emphasizes home and primary care and has an acute care bed ratio of 2.4 per 1,000 people. Following that example, Calgary at a population of two million would ideally have 4,800 acute care beds “but equally important is staffing those beds.”
Because so much health care is specialized, many services need to delivered in major urban centres, meaning “the whole province depends on Edmonton and Calgary,” said Sherman.
The province, he said, has taken some steps to remedy the provincial shortage of physicians by training more of them in rural areas.
Article content
He was referring to new medical schools in Lethbridge and Grande Prairie whose wider aim is to create 210 medical seats throughout the province over four years.
Other new training spots are also in Calgary but Sherman said funding cuts to post-secondary institutions in recent years don’t bode well for meeting the challenge posed by a civic population 25 per greater than the current count.
“You shouldn’t be cutting post-secondary (spending) — you have to create a system you retain your workforce and create your own,” he said.
“You’ve got to get ahead of the curve.”
Sherman insisted a key to a sustainable health care future in larger Calgary — one recited by other experts — is to unblock an acute care logjam by moving seniors and others who shouldn’t be in hospital to long-term care.
But that has to include more support for families, enabling them or professionals to care for elderly loved ones at home, he said.
“The whole problem is a flow problem but before you build more long-term care (facilities), invest heavily in home care,” said Sherman, adding a home environment is one-seventh as expensive as hospital care.
Dr. Max Jajszczok agrees, saying Alberta needs to adapt its health care system faster than other jurisdictions due to its aging and growing population.
“The amount of impact is going to be felt more than anywhere else but what Alberta has going for it is a younger population,” said Jajszczok, an adjunct assistant professor at the University of Calgary’s Cumming School of Medicine.
Article content
“Where the constraints will be is in (the number of ) specialty services, registered nurses and emergency departments — it’s going to be a tough change.”
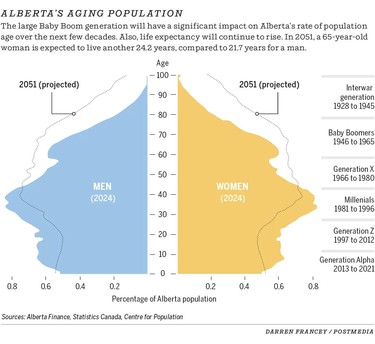
The number of seniors in Calgary is projected to increase from 268,000 this year to 371,000 by 2036 and to 483,000 a decade after that, he said. Those aged 85 years and over will jump from 25,000 to 44,000 in the next 10 years, he added.
There’s no way the province can build enough spaces to accommodate that demographic wave, hence the need for more community and home-based care, said Jajszczok.
Family caregivers need to be supported with tax breaks and more leniency from employers when those care needs arise, he said, and when that work is calculated to be worth nearly $90 billion annually in Canada, “it’s like a silent workforce,” he said.
“Home care needs to continue to grow at a rate much faster than the rest of the health system, this is the best way to support aging at home.”
“People, policy makers, social service policy makers, such as those who are responsible for municipal operations should be asking, what is the rate of growth in home care services over the next five years for Calgary, is this keeping with population growth and demand?” said Jajszczok.
And beyond that, there will be a significant increase to the number of people who will have dementia, require services in hospitals, for cancer treatment, and a family doctor specializing in geriatrics, he added.
“This demographic change will have a direct impact on how the city looks and operates over the next 10 years, there will be stressors on all programs serving this sector and population,” said Jajszczok.
Article content
In its workforce forecast, Alberta Health Services said family physician numbers for the Calgary zone will grow by 43 per cent by 2033 with those specializing in elder care by far the largest cohort.
Reflecting the aging demographic, new senior care family docs will number nearly double that of replacement recruitments, it said.
At the same time, 1,500 specialist physicians are expected to be recruited by 2033 in the Calgary zone, 578 of those new with the rest replacing retiring or departing doctors.
According to the Alberta Medical Association, there were 1,640 of its members with student status in 2024, a number that dropped slightly the following year, to 1,564.
AMA membership in the Calgary Zone in 2023 numbered 4,606 physicians, a number that’s risen steadily to 5,125 as of mid-February.
Last month, the province said it’s committed to spending $450 million to recruit and train doctors, who it says now number 13,700 throughout Alberta, though not all are necessarily currently practising. That number is 34 per cent more than a decade ago and includes 6,363 family physicians, they say.
That $450 million is part of a $7.7 billion in upcoming provincial spending that mainly addresses physician compensation.
All of those doctors are badly needed because of increasingly complex needs, physicians tend to see fewer fewer patients, “so now you’ll need more physicians, it takes more than one physician to replace a retiring one,” said Jajszczok.
Article content
While primary care networks — where family doctors coordinate with medical specialists to improve and streamline care — are a reality in Alberta, it’s an approach that needs to be employed more to better serve a larger population, said a U of C health care economist.
“We need to think about team-based care, it’s been very doctrinaire hospital-focused,” said Dr. Braden Manns. “A doctor who’s looking after 1,500 patients could work for 3,000.”
Another way to address understaffing magnified by population growth is the use of AI for triage and diagnoses in which patients input their symptoms for a quick, initial recommendation, he said.
Studies of the technology, now used in Ontario, shows it’s accurate and safe, said Manns.
 Dr. Braden Manns is pictured with a model of a kidney at his office in Calgary, Alberta on September 27, 2012. Photo by Leah Hennel
Dr. Braden Manns is pictured with a model of a kidney at his office in Calgary, Alberta on September 27, 2012. Photo by Leah Hennel
The province, he said, hasn’t committed to long-term health care planning for the Calgary area and are therefore “building for current needs, not future needs.”
“We need a comprehensive plan in what our needs will be in 10 years . . . they know how many family doctors, how many specialists they need, they know where the pain points are.”
There was a time earlier this century when the province did just that, said Manns, but current planning “is based on maintaining the current model of provision.”
“The question is ‘how do we change our service model because we can’t just build new hospitals.”
The UCP government said its Acute Care Action Plan is moving toward adding 1,100 acute care beds in Edmonton and Calgary, 400 of them at the South Calgary Health Campus.
Article content
No timeline for those projects was given and emergency doc Sherman said it would mean “we would still be far behind where we need to be today, let alone five years from now.”
That announcement of new beds made last November comes alongside a 50-year capital and long-term workforce strategy “to ensure the system can meet current and future health care needs,” Kyle Warner, spokesman for the Hospital and Surgical Health Services Ministry.
The province has earmarked $2 million to plan an expansion of the Alberta Children’s Hospital that will add 40 acute care and 10 mental health beds, a 32 per cent increase in capacity.
“The government has also invested $15 million in planning to build eight urgent care centres across the province to reduce wait times, improve outcomes, and ease pressure on hospitals, including a new urgent care centre in east Calgary,” said Warner.
Said Hospital and Surgical Health Services Minister Matt Jones: “It creates a foundation for sustainable, long-term change.”
Filling growing nursing need
The demand for nurses is so great, Bow Valley College is turning to a virtual training simulator to ensure it’s educating enough of them.
Enrolment for the college’s nursing programs is up by 10 per cent over the previous year and that’s only the start, said Dr. James Reddy Kakulavaram, the college dean of health sciences.
“Very few programs have waiting lists so it indicates a high demand.”
They’re working toward creating a health care centre of excellence that will grow the current full load equivalent students from the current 2,500 to 11,000 by 2035-2036, while tripling the number of annual graduates, he said.
Article content
BVC’s currently developing 14 new health care program areas on top of the six programs and eight courses offered now.
“Seeing that population growth, we’re moving towards that centre of excellence,” said Kakulavaram.
 Dr. James Reddy Kakulavaram, Associate Dean of Health Sciences at Bow Valley College, was photographed on Monday, March 2, 2026 in one of the hospital settings used to train nursing students at the downtown Calgary campus. Photo by Brent Calver/Postmedia
Dr. James Reddy Kakulavaram, Associate Dean of Health Sciences at Bow Valley College, was photographed on Monday, March 2, 2026 in one of the hospital settings used to train nursing students at the downtown Calgary campus. Photo by Brent Calver/Postmedia
“We have a 13,000 nurse shortage in Alberta and if the current trend continues to 2033, we’ll have a big deficit.”
He pointed to a provincial occupational outlook that forecasts a cumulative shortage of registered and registered psychiatric nurses for Alberta totalling 13,841 by 2033.
The college is also working to double its health care aid program while expanding instruction in recreational therapy and pharmacy technicians, he said, “but nursing is the centrepiece.”
But there’s a limit to the number of clinical spots for students’ hands-on experience and that employing virtual simulators is filling 30 per cent of those hours, he said.
“That’s allowing our students to enter the workforce sooner and address health care needs,” said Kakulavaram, whose BVC is the country’s largest user of the technology.
Research shows one hour of simulation can replace two hours in clinic by eliminating the wait for busy physicians and individual cases be assigned by the technology, says BVC, which places 700 students in real-life settings each year.
Some of those studies include licensed practical and psychiatric nurses, the latter reflecting a huge demand in the specialty, said Kakulavaram.
Helping meet that demand means credentialling international nurses, he added.
Article content
 Nursing students learn in a simulated hospital environment with a high-tech dummy at Bow Valley College’s downtown Calgary campus on Tuesday, February 24, 2026. Photo by Brent Calver/Postmedia
Nursing students learn in a simulated hospital environment with a high-tech dummy at Bow Valley College’s downtown Calgary campus on Tuesday, February 24, 2026. Photo by Brent Calver/Postmedia
“There’s a gap between getting a licence and getting employment and we can give them that Canadian way of a hospital setup,” said Kakulavaram.
According to the Canadian Institute for Health Information (CIHI), Alberta had the second-lowest rate of active nurses who were working full time in 2024 — 44.1 per cent, which was 21.5 per cent below the national average.
The number of internationally educated nurses in Alberta rose from 8.6 per cent in 2015 to 12.7 per cent in 2024.
In a nod to a ballooning demand, BVC on Feb. 20 announced the approval of the province’s first psychiatric diploma program allowing experienced practical nurses to complete that specialty faster than before.
Prof. Joseph Osuji has also been watching the population growth of the city and province with concern.
“We are so much anticipating that, our strategy speaks to that . . . the population is increasing and that means increasing (patient) complexity,” said Osuji, director of the School of Nursing and Midwifery at Mount Royal University.
What he sees in local schools’ ability to meet the demand for those positions doesn’t fully instill confidence, he said, though strides have been made.
But Osuji said provincial funding that added 32 nursing seats a few years ago is coming to an end at a crucial time.
“The province has been supportive of our dream to train nurses and midwives but we would like more,” he said. “We had an expansion but that’s coming to an end and we’re going back to our original number of 215 (registered nursing) seats.”
Article content
MRU, he said, can “easily” train 400 to 500 nursing students a year.
That instruction includes expanding the roles of registered nurses and licensed practical nurses while also completing the qualifications of international midwives, he said.
The program would also like to expand its training of midwives, whose active ranks number fewer than 200 throughout the province, said Osuji, whose school now turns out 15 a year.
Cancer centre sees surging demand
Like anyone with a new cancer diagnosis, Calgarian Nanette Gretton was overwhelmed by the prospect of what might lay ahead.
Last December, she received the bad news she has breast cancer but that anxiety was tempered somewhat by knowing the still-new Arthur J.E. Child Comprehensive Cancer Centre and its staff was her lifeline.
“I felt lucky we have this in our city, I think of the people who have to travel here,” she said. “It’s this beautiful place, you feel it’s really top notch.”
She said a biopsy procedure following her diagnosis went quickly and smoothly, creating the impression “I’m in a really good place.”
But Gretton said a subsequent consultation there in late January seemed rushed and left a more troubling impression.
“I had a whole lot of questions that weren’t answered,” said the 56-year-old.
“I guess they’re doing their best — maybe they just don’t have enough staff.”
 Nanette Gretton, a patient of the Arthur J.E. Child Comprehensive Cancer Centre, was photographed in Calgary on Friday, February 20, 2026. Photo by Brent Calver/Postmedia
Nanette Gretton, a patient of the Arthur J.E. Child Comprehensive Cancer Centre, was photographed in Calgary on Friday, February 20, 2026. Photo by Brent Calver/Postmedia
Dr. Don Morris admits to being nervous about meeting the cancer needs of a Calgary of two million people.
Article content
The medical director of the Arthur J. E. Child Comprehensive Cancer Centre said patient demand since the facility opened in October 2024 came as somewhat of a surprise.
“We’ve tried to stay on top of that but the migration to the Calgary catchment area was a bit of a shock,” said Morris.
“Some areas (of treatment) are tighter than others but it’s a bit of a perfect storm . . . that population that require a hospital stay in initial treatment has caught us off guard and continues to increase.”
When it was designed, he said the sparkling facility on the Foothills Medical Centre grounds was built for a projected 2040 capacity.
“It was said at one time it’s very over-built and we still have room to grow but does that 2040 now translate to 2031? Maybe.” said Morris.
“For radiation medicine we still have some capacity and shell areas we could put in new machines but that would require capital dollars.”
Currently, of the centre’s initially-allotted 160 inpatient beds, 94 are currently funded for use and are already at 105 per cent capacity, he said.
To keep pace with growth would require adding 10 to 15 beds per year, said Morris.
Morris said he’d like to see some treatment programs such as cardiac and head and neck cancer that are located at other hospitals in the city moved to the Arthur Child “but we don’t have the resources at this point in time.”
The centre also serves patients who live throughout southern Alberta, where there are regional clinics that do provide cancer care and increasing their capabilities can take current and future pressure off the Arthur Child, said Morris.
Article content
For now, the centre is holding its own, he said, bolstered by the recruitment of 130 nurses in the past four months and 15 new oncologists in the last two years.
That, and improved triaging has led to a recent reduction in wait times at the Arthur Child, said Morris, but it’s a constant struggle to hold the line.
“We’re never fully there (on staffing) and if we hadn’t been really aggressive with hires we wouldn’t have this optimism,” he said.
“If we put our heads in the sand, we would not be ready . . . it’s a testament to the staff that we’re weathering the storm.”
 Dr. Don Morris, medical lead for the Arthur J.E. Child Comprehensive Cancer Centre, speaks at an event announcing a $5 million donation by ARC Resources to the Alberta Cancer Foundation’s OWN.CANCER campaign at the centre in Calgary on Tuesday, March 12, 2024. Photo by Brent Calver/Postmedia
Dr. Don Morris, medical lead for the Arthur J.E. Child Comprehensive Cancer Centre, speaks at an event announcing a $5 million donation by ARC Resources to the Alberta Cancer Foundation’s OWN.CANCER campaign at the centre in Calgary on Tuesday, March 12, 2024. Photo by Brent Calver/Postmedia
One bright spot for future medical demand is that the incidence of cancer in the country has been falling annually — by 1.2 per cent for men and 0.4 per cent for women — since 2011, according to the Canadian Cancer Society.
Survivability has also improved with 64 per cent of cancer patients now living five-plus years after diagnosis compared to 25 per cent in the 1940s.
While that’s welcome news, Morris said the latter statistic means more demand for his services.
“It’s double-edged sword. People are living longer and better but they still have cancer and need to be continually seen,” he said.
Looking ahead to serving a Calgary of two million people, Morris sums it up by saying he’s “concerned given the number of new treatment strategies that involve some inpatient care in addition to the population growth.”
New patient Gretton said her medical plan that will include surgery, radiation and hormone therapy puts in perspective for her the importance of ensuring a responsive, timely cancer program in a growing Calgary.
Article content
“I worry about that, if it already takes as long was what I’ve been seeing,” she said.
And there’s something more personal she hopes won’t be lost at the Arthur Child in a larger city: the compassionate, thoughtful care she said she’s received in most of her visits.
Physicians warn of strain amid health overhaul
Ensuring the needs of a two million-strong Calgary are met are daunting enough, says the head of a group representing physicians in the city.
The provincial government’s dramatic health care reforms that include creating four new health ministries, allowing more medical responsibilities to non-physician players along with increasing privatization only adds to the uncertainty, said Dr. Catherine Macneil, president of the Calgary and Area Medical Staff Society.
“I worry whether the restructuring is going to help the coordinated approach over different health care corridors,” said Macneil.
“I worry about undermining the medical home by using other people (like pharmacists), saying they can do the same things . . . it’s the functioning in isolation that’s worrisome. We don’t know what (the reforms) are going to be — it’s a risk trying to make all the providers equivalent.”
She describes the medical home as a seamless collaboration between physicians and other care providers ranging from pharmacists, licensed practical nurses and dieticians.
Similarly, Macneil said opening up more of the medical system to private, for-profit surgical providers that’s funded publicly won’t meet the requirements of a fast-growing city given there’s already a limited and stretched workforce. The province has also said it intends to allow physicians to practise simultaneously in the public and private systems.
Article content
“The bottleneck isn’t surgeons unwilling to do surgeries, it’s the post-operative care and you can include (a higher) number of hip replacements but it reduces the number of anesthesiologists (in public settings),” she said.
“You can’t rob Peter to pay Paul.”
The UCP government says contracting out more surgeries will reduce waiting lists in the public sphere while its spinning off four separate ministries from one and reducing the role of Alberta Health Services will make the system more responsive to patient needs.
“We’ve actually turned our hospitals into multi-purpose facilities and taken them away from their core job, which is to deal with emergencies and to efficiently make sure that people can get surgery and also do the convalescence there,” Premier Danielle Smith said last May.
“We’ve tried it that way, all integrated. I think we need to try it a different way, because it clearly wasn’t working.”
Macneil, who’s a pediatrician, said the key reducing future health care demand is ensuring the health and welfare of pregnant moms, babies and children.
“There’s a saying that ‘the years before five last the rest of our lives,’” she said.
While more can be done in preventative health, home care and a team approach, said Macneil, there’s no way the city’s demands can be met without an increase in infrastructure.
As for an ideal number of physicians for Calgary a decade from now, she said that calculation isn’t easy to make.
“I don’t know if we have quite enough now — it’s easy to say we’ll need 25 per cent more doctors, maybe we do. I don’t know,” said Macneil.
And while increasing the number of physician training spots in universities is clearly vital, the payoff is much delayed, with that education lasting eight to 15 years, she said.
![]()
Article content
Share this article in your social network