
The occurrence of frailty in Chinese older adults in the present study was 27.19%. Frailty is closely related to the occurrence of falls, fractures, and death. Hence, identifying high-risk individuals is important to prevent frailty and associated adverse outcomes, especially in the older adults. The results of this study reveal that advanced age, low BMI, debt, living in the countryside, cataract, family type, history of alcohol consumption, level of social support, depressive symptoms, and neighborhood relationships are all key factors influencing the frailty of older adults. However, as this research is a cross-sectional study, it can’t establish causality. Future research should focus on these factors through cohort studies to verify their causal relationships with frailty in older adults, thereby providing a scientific basis for improving the health outcomes of the elderly.
This study revealed that age was a predictor of frailty in the older adults, which is consistent with previous findings [20]. This may be attributed to age-related biological changes, such as a decrease in basal metabolic rate, organ aging, or even a decrease in muscle strength. All of these may result in a decline in physiological functional status. In addition, studies have found that aging may trigger inflammatory responses and neurodegenerative diseases, which reduce skeletal muscle mass and strength, in turn inducing frailty [21].
Living in the countryside was considered an important aspect of the diagnosis of frailty. The previous study also came to the same conclusion [22]. A meta-analysis [23] showed that the incidence of sleep disorders in rural areas in China was generally higher than in cities because of the working habits and low economic income. Poor sleep quality can cause a series of physical and mental problems, which may eventually lead to frailty. Carmen’s study [24] demonstrated that insomnia is related to anxiety, chronic pain, and fatigue. All of them were important components of multidimensional frailty, and the decline in sleep quality was more likely to lead to frailty. These findings suggest that providing sleep-promoting interventions to older adults with sleep disorders may improve frailty.
This study also found that cataract was an independent predictor of frailty. Cataract is the primary cause of vision loss and blindness in the older adults, which may significantly increase the risk of fall [25]. Falls have already been proven to be an independent influencing factor for frailty. Studies have shown that the skeletal muscles of patients who have experienced falls were weaker. Such patients may also experience fear, thereby rejecting exercise to a certain extent. In such cases, the patient’s white matter atrophy rate increase, thus increasing the risk of frailty [26].
The study also found that alcohol consumption may decrease the incidence of frailty in older adults. However, this finding contradicted the results of previous studies [4], which showed that alcohol consumption increased the risk of frailty. Due to cultural and consumption patterns, unlike the red wine consumption common in other countries, Chinese residents, particularly the elderly, often consume baijiu, a spirit primarily made from fermented grains. This type of alcohol is typically consumed during meals, which may help balance intake and reduce the direct impact of alcohol on the body. Moreover, moderate baijiu consumption in social settings can potentially alleviate stress, which might have a positive effect on health.The observed difference in frailty risk could also be attributed to the amount of alcohol consumed. Research suggests that moderate alcohol intake can be beneficial for health, as low levels of ethanol may enhance the immune response [27]. In addition, the lack of detailed data on alcohol consumption patterns, such as the type of alcoholic beverages consumed, the frequency of consumption, and the quantity consumed per occasion, lead to no further analysis of alcohol consumption was performed in this study, which may be also a direct cause of this result. Future studies should consider incorporating more granular data on alcohol consumption to better elucidate its impact on frailty.Secondly, the cross-sectional design of our study precludes the establishment of a temporal relationship between alcohol consumption and frailty. This design limitation means that we cannot determine whether alcohol consumption precedes the onset of frailty. Longitudinal studies are needed to address this issue and to provide more robust evidence on the causal relationship between alcohol consumption and frailty in older adults.
The results showed low BMI were susceptible to frailty, which is consistent with the research views of other scholars [28, 29]. Low BMI is associated with an increased risk of chronic disease, malnutrition, and sarcopenia, all of which increase the risk of frailty. However, the current relationship between frailty and BMI remains controversial. Studies [30] have shown that every unit increase in BMI results in a 12% increased risk of frailty. Furthermore, a meta-analysis suggested [31] that patients with a high BMI were more likely to be debilitated than those with a normal BMI. The above results suggest that future studies should investigate the relationship between BMI and frailty at different stages.
Moreover, the results of this study suggest that debt is an independent risk factor for frailty in older adults. In this study, debt refers to chronic debt such as housing loans and medical loans. Debt itself has recently caught the attention of researchers as a unique stressor [32]. A growing body of literature links severe or chronic debt, unsecured debt, unsecured debt, and chronic financial stress to cumulative physiological stress. Financial stress leads to differences in morbidity and mortality, in part because debt-induced stress increases the risk of obesity, substance abuse, depression, suicide, and poor self-health [33, 34]. The above outcomes are closely related to the occurrence and development of frailty. Nevertheless, other pieces of research showed contradictory results. In a study of 17 European countries from 1995 to 2012, Clayton [35] found that while long-term total household debt was associated with poor health outcomes, short-term total household debt predicted positive health outcomes. Their findings suggest that the health impact of total household debt depends on its form, which may also be true at the individual level.
The present study [30] also found that depression was associated with frailty, which is supported by previous studies. This may be due to the depression predisposes dopaminergic neurons that are continuously under oxidative stress and highly bioenergetic to cellular stress, resulting in mitochondrial dysfunction and reduced adenine nucleoside triphosphate production. The decreased dopaminergic system function leads to motivational deficits, disability, and slowing of movement, thereby inducing frailty [36]. Studies [37, 38] have also found that depression may induce loss of interest, memory loss, social interaction avoidance, and declined social participation in the older adults, which is also a major reason for the occurrence of frailty. Therefore, clinical medical staff should pay attention to the psychological state of older adults, which is of great significance for improving the patient’s debilitating condition.
Moreover, this study found that frailty is closely associated with social support. The scores of social support in the frail group were significantly lower than in the non-frail group. Social support was not only measured by the Perceived Social Support Scale, but was also analyzed by family type and neighborhood relationships. The results of this research are supported by previous studies. Anantapong’s study [39] of older depressed patients showed that social support was significantly associated with frailty. The reason may be that social support plays an important role in the physical and mental health, and a good level of social support can enable individuals to obtain positive emotional experiences and stable social feedback, which can reduce the impact of negative life events on the health of older adults, and improve the mental health of the them [40]. Old people crave the company of their children. However, young people are forced to go out to work to make a living and must leave the older adults to live alone for extended periods of time. Harmonious neighborhood relationships can resolve the loneliness of the older adults, promote the participation of the older adults in social activities, actively exercise the body, improve their ability to cope with diseases, and improve frailty [41]. A large difference in frailty was observed between the Dinker family and the Main family. Traditional research [42] has shown that having children was associated with more family support, emotional comfort, and life care. Good family support promotes a good physical and mental condition. In the future, children should be called upon to provide more care, and more attention and organizational care should be given to the lonely older adults at the community and social levels.
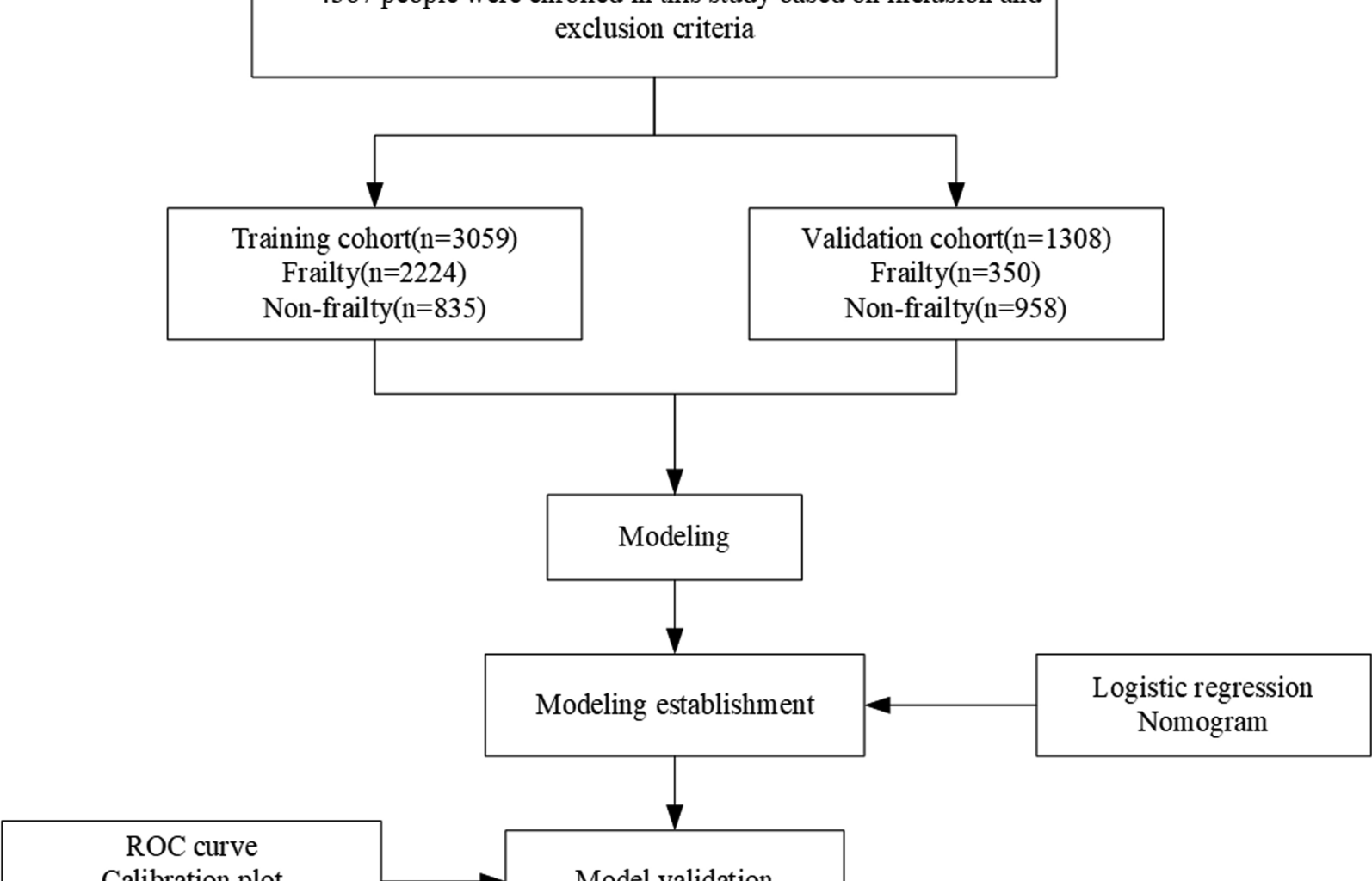
The risk factors influencing the prognosis of frailty were determined through univariate and multivariate logistic regression analyses. The nomogram was used to visualize the identified risk factors, thereby enabling the prediction. The internal verification results show that the model has high degrees of discrimination and calibrated accuracy. The accuracy and high consistency with actual incidence data highlight its value for clinical applications. Nevertheless, the limitations of this study should be acknowledged. Our model was developed and validated based on population data from China, and cannot be directly extrapolated to other ethnicities. Furthermore,this study utilizes a cross-sectional design, enabling us to identify associations between various factors and frailty at a single point in time. However, this design does not support causal inference. Our data collection reflects the prevalence of frailty among older adults, capturing their health status as it stood at the moment of data gathering. A critical limitation of using cross-sectional data is the inability to anticipate future frailty occurrences. We acknowledge this limitation and recommend that future studies employ longitudinal data to develop models that can more accurately predict the incidence of frailty. Additionally, longitudinal designs are essential for exploring causality and understanding the temporal sequence of these associations. In addition, our nomogram model has been internally validated, with acceptable levels of discrimination and calibration. Nonetheless, to confirm the model’s generalizability, external validation in diverse populations or prospective cohorts is necessary. This step is crucial for assessing the model’s applicability and reliability across different settings and populations. While our sampling strategy was designed to minimize selection bias and ensure representativeness, the analysis may still be limited by regional differences in healthcare access, particularly between urban and rural areas, which could influence the prevalence and risk factors of frailty. The most prominent strength of this study is the large sample size. The present study can be used to assess the risk of frailty in older Chinese adults, as well as for preventive interventions targeting variable risk factors, with good guiding implications in public health and clinical settings. Future studies should aim to validate the model in these underrepresented subgroups to ensure its applicability across diverse populations within China.