
Cancer is the leading cause of death in Ireland, so how the country performs on every aspect of the disease, from prevention and screening to treatment and survivorship, is of critical importance.
Each diagnosis is a personal story for the one in every two people who will develop cancer in their lifetime, but population-wide analysis shapes their care. The National Cancer Registry of Ireland (NCRI) has been collecting and classifying information that informs policymakers and researchers for more than 30 years. This feeds into comparative international data that gives a broad sense of what sort of country this is for cancer patients.
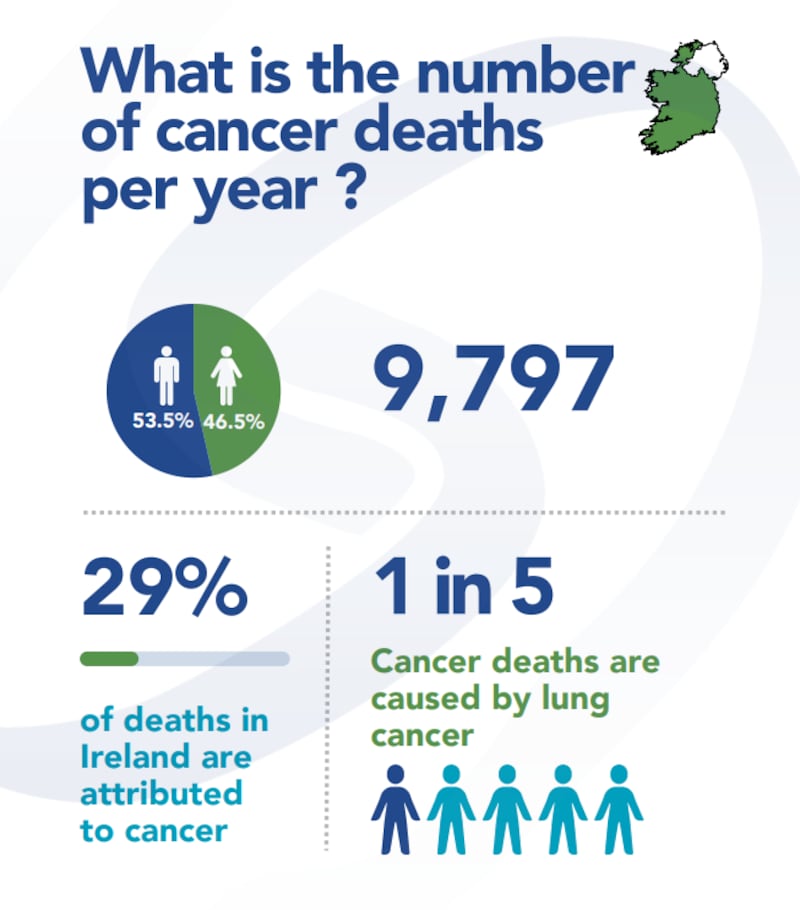
Ireland has the third highest mortality rate for this disease in the EU, according to country cancer profiles published last year. About 10,000 people died of cancer here in 2024.
While Irish cancer mortality rates are still 5.4 per cent higher than the EU average, rates have improved significantly in recent years, says the HSE in a written response to The Irish Times: “Between 2011 and 2021 cancer mortality decreased by 21 per cent among men and 16 per cent among women, surpassing reductions seen in countries that are our economic peers.”
The European Cancer Inequalities Registry notes that new cancer diagnoses here were the second highest in 2022 (behind Denmark). However, this finding should be considered in the context of high levels of data completeness provided by the NCRI, says the HSE. The three countries with the highest cancer incidence in the EU27 (ie, Denmark, Ireland and the Netherlands) are all countries that have cancer registries providing national coverage, while in some other countries estimations are based on data pooled from regional registries.
While the EU profile of Ireland acknowledges progress in opening rapid access clinics and reducing waiting times, much more needs to be done, says the Irish Cancer Society (ICS). The society “hears from people across the country, day-in and day-out, anxious that they are waiting far too long to get an appointment for a cancer test, or for their cancer treatment once they have received a cancer diagnosis”, says policy and campaigns manager Emma Harte.
“In recent years, we know that thousands of people didn’t get into their first chemotherapy or radiation therapy appointment within the recommended timeframe. We know that too many people were waiting longer than they should have to get surgery for prostate, lung or breast cancer.”
The good news, she says, is that “today, two in three people will survive their cancer diagnosis, compared to roughly one in two in the mid-1990s”. This improvement is attributed to targeted investments in staff and infrastructure, led by 10-year national cancer strategies.
The first, which was published in 1996, reorganised services and achieved a 15 per cent reduction in the death rate from cancer in the under-65 age group within eight years. The National Cancer Control Programme (NCCP) was established as part of the second strategy, and the third (2017-2026) runs to the end of this year. The ICS, which has called for clarity over plans for the next strategy, has consistently highlighted the lack of ringfenced funding for the strategy now in place. This, it says, has caused staffing shortages, outdated cancer care equipment, and a lack of progress reporting on defined targets.
 Statistics: National Cancer Registry Ireland
Statistics: National Cancer Registry Ireland
Ireland’s national cancer control planning, via successive strategies, is in the top rankings globally, according to an international study led by Queen’s University, Belfast, which was published in the Journal of Cancer Policy in February. Researchers reviewed national cancer control plans for 20 countries, ranking each one on the full continuum of cancer care – including prevention, early detection, diagnosis, treatment, rehabilitation, palliative care, and research. It found Ireland ranks first overall.
The HSE says there has been a more significant decline in rates of avoidable cancer mortality compared to the EU average. For example, in the case of lung cancer, between 2011 and 2021 rates decreased by nine per cent among women (compared to a four per cent increase across the EU) and by 31 per cent among men (compared to a 27 per cent decrease in the EU).
The ICS looks to Denmark as a good international comparison with Ireland in terms of access to cancer services and patient outcomes. Denmark’s population of six million is only slightly larger than the Republic’s 5.4 million, and its reported cancer incidence is higher. Both countries invest similar amounts in healthcare per person (€385 in Denmark; €382 in Ireland, according to OECD data).
In Denmark, most people waiting for cancer tests and treatment are seen on time. The Danish National Audit Office found that six per cent of cancer patients did not get treatment within the required 14 days, between 2019 and 2023. By April and June 2024, practically all (99.8 per cent) cancer-related tests or treatments were delivered within the recommended timeframe. Ireland, however, is failing to reach targets that are lower.
The aim here is that 90 per cent of patients start radiation therapy within 15 working days of being deemed ready for this treatment. Just 78.7 per cent of people were seen within that recommended timeframe last year, according to an NCCP response to a Dáil question. The performance on receiving a first chemotherapy cycle was slightly better, with 85 per cent of cases meeting a similar target.
[ Ireland found to be worst in Europe for availability of new cancer treatmentsOpens in new window ]
In Denmark, the five-year, all-cancer survival rate increased between the periods 2002-06 and 2017-21 from 59 per cent to 74 per cent for women and from 54 per cent to 72 per cent for men.
In Ireland, the five-year, all-cancer survival rate rose from 57 per cent among those diagnosed between 2004 and 2008 to 65 per cent among those diagnosed between 2014 and 2018.
The ICS highlights several factors in Denmark’s better patient outcomes.
Firstly, a person there diagnosed with cancer has a right to start treatment within 28 days of referral and must start treatment within 14 days of consenting to their treatment. If a patient cannot access treatment in their region within that time, an alternative option has to be provided.
Denmark has a much larger supply of equipment necessary for cancer care, such as CT scanners (256 compared with 102 here, according to 2022 figures) and PET scanners (52 v nine). However, Ireland has more MRI units: 87 compared with 54.
There is disparity in access to the latest drugs, with 69.2 per cent of new cancer medicines for breast and lung cancer being reimbursed in Denmark compared with 38.5 per cent here. Denmark also launched three times as many clinical trials as Ireland annually (75 compared with 25) between 2018 and 2023. Its healthcare system has one of the most advanced digital infrastructures in the EU, whereas Ireland has made the least progress in this regard.
 Orla Dolan, chief executive of Breakthrough Cancer Research. Photograph: Leon Farrell/Photocall Ireland
Orla Dolan, chief executive of Breakthrough Cancer Research. Photograph: Leon Farrell/Photocall Ireland
Clinical trials are important because they enable early access for patients to the latest drugs, at no cost to the State, says Orla Dolan, chief executive of Breakthrough Cancer Research. “Also, when somebody’s on a clinical trial, they’re so tightly managed, the care around them is generally higher.”
She believes bureaucracy and very strict interpretation of issues such as GDPR has hampered Irish participation in trials – or protocols, as some clinicians prefer to call them, as they can be a new way of using well-established medicines. However, she acknowledges that blocks in the system are being identified, with a view to speeding up trial approvals.
Breakthrough Cancer Research raises and grants about €4.5 million annually, mostly on seven types of cancer that have the poorest survival rates: lung, brain, liver, oesophageal, stomach, ovarian and pancreatic. There is a globally interconnected drive to find cures for cancer, in which this country plays a significant part.
“Good ideas have no borders,” says Dolan, with research on the role of the immune system in cancer “a very big strength here”; also systems biology and the development of precision medicines. “There’s a lot of work being done on early detection and biomarkers, where we’re kind of leading the way in those,” she says.
A highly educated workforce and interconnected health system are some of Ireland’s advantages, while challenges include the lack of a career path for postdoctoral researchers and the current state of biobanking – ie, collection and storage of samples of blood and tissue for studies.
We know that in research-active hospitals and environments, people will do better generally, even if it’s not in cancer, “because it’s just an ethos”, says Dolan, who hopes that research will be a more integrated part of the next cancer strategy. In a hospital setting “research is a core component of everybody’s job”, she adds.
A significant socio-economic dimension to cancer deaths in Ireland has been flagged by the European Cancer Inequalities Registry. Individuals living in the most deprived areas faced, on average, a 43 per cent higher risk of mortality within five years of diagnosis compared with their counterparts in the least deprived regions. The HSE says the current national cancer strategy “has a key focus on narrowing the disparity”.
The EU report also notes that Ireland outperforms most countries in managing risk factors, “particularly excelling in tobacco control policies. Over the past decade, the country has seen reductions in the share of daily cigarette smokers, in alcohol consumption, and in prevalence of overweight and obesity”.
Childhood cancer
Every distraught parent of a child who has been diagnosed with cancer in Ireland wants to know: will they receive treatment that is on par with healthcare elsewhere?
“Absolutely,” says Prof Owen Smith, consultant paediatric haematologist at Children’s Health Ireland (CHI) and professor of child, adolescent and young adult oncology at Trinity College Dublin. However, he suggests areas for improvement could include the opening of a proton radiation therapy facility in Ireland and a greater focus on survivorship.
Proton therapy, which is available in 11 European countries, is a very precise form of radiation which causes less collateral damage than the more usual photon therapy used here. The latter “doesn’t just hit the tumour, it hits the surrounding tissues”, he explains, whereas proton therapy is targeted to the cancer and there are very few knock-on for the surrounding tissue.
Smith and his colleagues in CHI@Crumlin, the national centre for paediatric cancer, sends some patients to England or Germany for proton therapy, but he believes it needs to be available here. He acknowledges that a group within the HSE’s National Cancer Control Programme – for which he is clinical lead for children, adolescent and young adult cancers – has been looking at the feasibility of establishing a proton therapy centre in Ireland, “but nothing has happened”.
 Owen Smith, professor of Child, Adolescent and Young Adult Oncology, Trinity College Dublin
Owen Smith, professor of Child, Adolescent and Young Adult Oncology, Trinity College Dublin
The next national cancer strategy will consider both patient-specific needs and technology-specific requirements, including the potential role of a national Proton Beam Therapy (PBT) service, the HSE tells The Irish Times. However, “at present, there are no confirmed plans, locations or timelines for the development of a PBT facility in Ireland”.
The other big area for the next cancer strategy, says Smith, is survivorship. About 85 per cent of children, adolescents and young adults now survive a cancer diagnosis, with many decades of life ahead.
“If you’re a five-year-old or a 25-year-old, it’s a different story than if you’re a 75-year-old,” he says. “We have to get survivorship better.”
This involves trying to anticipate the toxicities (harmful side effects of cancer treatments), that they will develop over time, and intervening to minimise them.
Smith is principal investigator with Magic-I, a five-year clinical study launched last May that is looking at how to use genetics, genomics and big data to optimise treatments in childhood cancer. “The genes that you’ve inherited from your mum and dad will predispose you to certain toxicities. This is really important, and we’re basically one of the forerunners in this whole area at the moment.”
CHI@Crumlin sees 200-210 children newly diagnosed with cancer each year. There is no distinction between public patients and families who have private health insurance, and there are no waiting lists, he says. There are about 170 new cancer cases annually among those aged between 16 and 24.
Smith is critical of the slowness in regulating the use of new drugs, especially immunotherapies that started to emerge in 2017. For example, when the European Medicines Agency approved the use of Car T-cell therapy, the UK got stuck in straight away, whereas it was three or four years before it could be used here.
“We were sending our children to Britain for these Car T-cell therapies. We cannot continue to do that. We have to align ourselves with Europe more,” he says.
For very rare childhood cancers, if there’s a treatment that has proven efficacy and which we cannot offer in Ireland, he adds – stressing “proven, not voodoo” – the treatment abroad scheme is “very good in facilitating or sending those patients to another country, if needs be”.