
The aim of this study is to assess the incidence and burden of myocarditis in the Middle East and North Africa region by analyzing age-standardized mortality rate (ASMR), age-standardized disability-adjusted rate (ASDR), and age-standardized incidence rate (ASIR) data from the Global Burden of Diseases Study 2019. The findings revealed a minor change in the ASIR of myocarditis over the three decades, while there was a notable decrease in both ASMR and ASDR during the same period. Across sex and age Groups, females exhibited a higher ASMR and ASDR compared to males, and lower ASIR. Myocarditis incidence varied among countries, with Iran, Qatar, and the United Arab Emirates showing the highest ASIRs in 2019, while Kuwait, the Syrian Arab Republic, and Libya experienced decreases since 1990. Oman, Iraq, and Egypt had the highest ASMRs, whereas Bahrain, Jordan, and Turkey had the lowest. The Social Demographic Index (SDI) appeared to have a neutral or marginally positive correlation with ASIR, while the correlation with ASMR and ASDR changed from negative to positive at certain SDI thresholds.
In comparison to the findings of the Global Burden of Myocarditis study, both our and global burden studies noted a decrease in the ASIR and ASMR over the three decades, indicating a potential improvement in myocarditis management and prevention efforts globally and regionally. The decline in disability-adjusted life years (DALYs) and ASDR observed in our study aligns with the slight decrease in DALYs reported in the global analysis. Moreover, we found that high SDI regions consistently showed a more ASIR of myocarditis compared to middle and low SDI regions. This suggests a potential association between higher socioeconomic development and increased incidence of myocarditis in the MENA region. Conversely, the global burden study observed a slight decrease in ASIR across all SDI regions worldwide from 1990 to 2019, indicating a different trend on a global scale. Additionally, the global study noted that middle SDI regions had the highest ASMR and ASDR in 2019, whereas low SDI regions had the lowest ASMR and ASDR. Both studies also observed higher age-standardized rates (ASRs) of myocarditis among males compared to females, with a downward trend in ASRs over time. However, our study emphasized specific age and sex Groups within the MENA region, highlighting older population as having the highest incident cases and deaths in 2019.
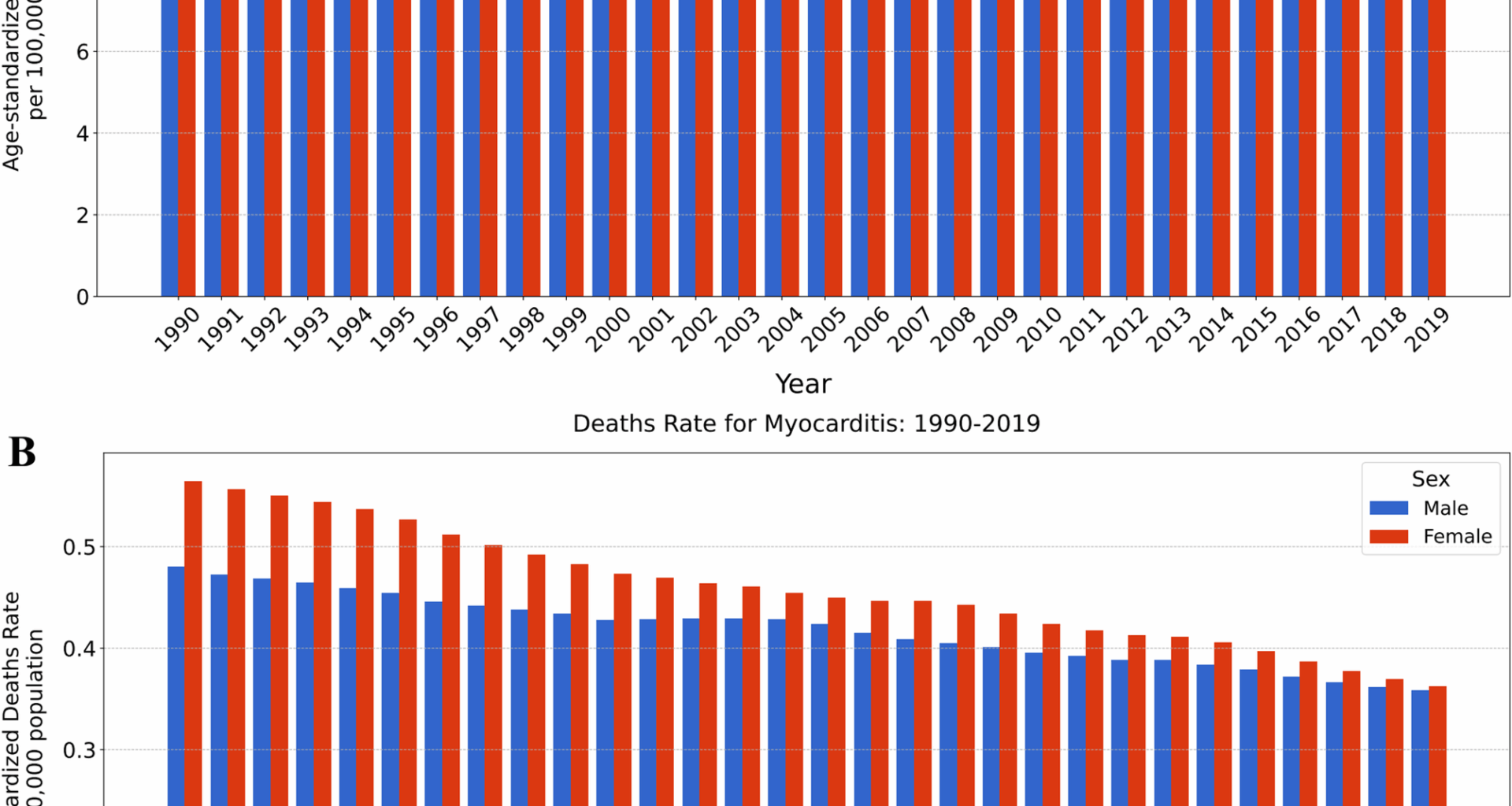
The lower ASIR of myocarditis in females compared to males may be attributed to several pathophysiological mechanisms. One potential explanation is the hormonal influence, particularly estrogen, which has been implicated in modulating the immune response and inflammatory processes. Estrogen receptors are present in various cardiac cells, and estrogen has been shown to affect myocardial remodeling and inflammation [25, 26]. Although females have a lower incidence of myocarditis, our results indicate that females have higher ASMR and ASDR than males. Various studies showed that females with myocarditis, especially after menopausal age, have a more severe presentation of myocarditis and experience heart failure symptoms (and higher NT-proBNP levels) and arrhythmias more often compared to males [27,28,29]. Females may also present with different clinical features (e.g., dyspnea vs. chest pain in males), potentially leading to delayed diagnosis or treatment [30]. Additionally, cultural and educational factors in the MENA region can influence women’s decisions to seek medical care, and adhere to treatments [31]. All these explanations could be contributing to higher mortality and DALY rates of myocarditis in females despite the lower incidence rate.
Understanding the differences in clinical manifestations, causes, and diagnostic approaches between pediatric and adult patients is essential for comprehending the burden of myocarditis across different age groups [32]. The causes of myocarditis vary by age [33]; however, we could not assess it due to a lack of etiological data for myocarditis in the GBD database. The observed high ASDR in neonates and newborns, may be explained by the immaturity of the neonatal immune system, rendering them more susceptible to infections, including viral myocarditis [34]. Previous studies have shown that fulminant myocarditis of unknown etiology is more frequent in children and particularly common in newborns with a poor prognosis [35]. Generally, the burden of myocarditis (ASIR, ASMR, and ASDR) rose steadily with advancing age in adults and increased sharply after the age of 70. Comorbidities such as hypertension [36], low ejection fraction [37] and cardiac arrhythmia [37] which are more prevalent in elder population and, age-related changes in cardiac structure and function may contribute to the increased burden of myocarditis in older age groups [38]. Additionally, the adverse effects of myocarditis, such as cardiomyopathy and cardiac arrhythmias, could cause severe complications in older cases and lead to a higher burden in this age group [39,40,41]. Moreover, dysfunction of the aging immune system and a decrease in estrogen signaling in postmenopausal women, which weaken the immune response, could possibly explain the increase in the incidence rate [42, 43]. While several studies—particularly previous GBD analyses and those using autopsy or endomyocardial biopsy—align with our findings regarding the increasing incidence of myocarditis with age [44, 45], many clinical observations report a different pattern, with higher incidence seen in younger adults [46]. These contrasting findings highlight the need for further, well-designed studies to clarify age-related trends in myocarditis incidence.
It is important to delve deeper into the specific reasons behind the observed differences in the burden of myocarditis across different countries in the MENA region as evident in disparities observed with other cardiovascular diseases in MENA region [10]. High ASIR in Qatar, United Arab Emirates, and Iran is characterized by higher socio-demographic development and healthcare infrastructure, likely exhibiting increased disease surveillance capabilities, leading to more accurate detection and reporting of myocarditis cases [47]. Additionally, lifestyle factors such as increased urbanization, sedentary lifestyles, and dietary habits prevalent in urban areas might contribute to a higher incidence of myocarditis. Decreasing ASIR in Kuwait, Syrian Arab Republic, and Libya may be attributed to improvements in healthcare access and infrastructure over the study period [48]. Enhanced preventive programs, sanitation, and public health awareness campaigns, may have contributed to a reduction in infectious causes of myocarditis, thereby lowering its incidence [49]. High ASMR and ASDR in Iraq, Egypt, and Oman may be in light of that these countries face challenges related to healthcare access, quality, and resource allocation, resulting in higher mortality and death rates from myocarditis [50]. Limited access to timely and appropriate medical care, including diagnostic facilities, intensive care units, and specialized cardiac services, could lead to delayed diagnosis and suboptimal management of myocarditis cases, thereby increasing the risk of mortality [51]. Conversely, low ASMR and ASDR in Bahrain, Jordan, and Turkey from myocarditis is because they have more robust healthcare systems, with better access to medical services and advanced cardiac care facilities. Timely diagnosis, effective treatment modalities, and comprehensive cardiac rehabilitation programs may contribute to improved outcomes and reduced mortality rates in these countries [52].
The study explored the relationship between the SDI and myocarditis burden. Initially, the ASIR remained relatively stable over the 30-year period, suggesting that the socio-demographic development of a country may not directly influence the incidence of myocarditis. However, there was a marginally positive correlation between SDI values, indicating that as countries reach higher levels of socio-demographic development, there may be a slight increase in the incidence of myocarditis. The ASMR and ASDR exhibited notable declines, indicating improvements in healthcare access, quality, and interventions, particularly in countries with higher SDI values. Interestingly, despite the relatively stable ASIR in MENA region, countries with higher SDI values, such as Qatar, the United Arab Emirates, and Iran, experienced increases in ASIR over time, suggesting potential shifts in disease surveillance, and reporting practices [53]. Conversely, countries with lower SDI values, such as Kuwait, the Syrian Arab Republic, and Libya, saw decreases in ASIR, possibly reflecting improvements in healthcare infrastructure and preventive measures. Although viral infections are the most common cause of myocarditis [3], autoimmune diseases, another major cause of myocarditis, are generally more prevalent in high-income countries [54]. Moreover, immune checkpoint inhibitors, essential drugs in cancer treatment, also represent an important cause of myocarditis [6] and, due to their high cost, access to these drugs may be limited in regions with a low SDI. Additionally, different clinical presentations of myocarditis, which range from mild symptoms of chest pain and palpitations to life-threatening cardiogenic shock and ventricular arrhythmia, could cause underdiagnosis, especially in low SDI countries that may have limited access to diagnostic methods such as cardiac magnetic resonance (CMR) imaging, and endomyocardial biopsy [2, 55]. However, the explanation of this trend based on the socio-demographic index is complex; these factors may lead to a higher incidence of myocarditis in high-SDI countries. Furthermore, the negative correlation observed between SDI and ASMR/ASDR up to a certain SDI threshold suggests that as socio-demographic development improves, mortality and death rates due to myocarditis decline. However, beyond a certain point (SDI around 0.72), the correlation turns positive, indicating that in highly developed regions, other factors may contribute to an increase in mortality and death rates, such as aging populations or changes in disease epidemiology [47].
The main Limitation on our analysis, in spite of the GBD 2019’s methodological advancements, was the attainability of source data. Inadequate reporting and data entry can cast doubt on the accuracy of the information gathered. Study results could be skewed by lack of access to high-quality data, which would reduce the strength of the evidence. In countries with lower SDI and continuous conflicts, the consequences of missing data might be more severe because fewer healthcare institutions might be conducting the epidemiological investigations. The other factor that challenges the accuracy of GBD data is the absence of longitudinal data on nonfatal myocarditis cases identified in cross-sectional studies which poses a significant challenge for precisely estimating the actual burden of myocarditis. Additionally, the heterogeneous clinical presentation of myocarditis, case definitions, and various assays, instruments, and diagnostic methods in the data collection stage could lead to over or underdiagnosis and affect the accuracy of GBD data. Also, the GBD database did not classify myocarditis based on its subtypes and underlying etiologies, such as infectious, immune-mediated, and toxic myocarditis. This could limit our understanding of this disease’s burden, especially when focusing on specific regions.