
Ureteric dissection is a rare and complex condition characterized by the separation of the ureter’s inner mucosal and middle muscular layers due to a breach in the damaged lamina, through which urine can seep into and result in the formation of a potential cavity. This condition, though infrequent, poses significant risks if not diagnosed and managed promptly [1].
The etiology of ureteric dissection is often linked to obstructive events at the distal end of the ureter. These obstructions can result from surgical iatrogenic injuries, where excessive traction or inadvertent damage occurs during procedures like nephrectomy or ureteral stenting. Alternatively, trauma or intrinsic or external compression from conditions such as large calculi or tumors can also precipitate this condition. Understanding the underlying causes of ureteric dissection is crucial, as these obstructions can severely impact the ureter’s structural integrity and functional capacity. The aim of this case was to describe the clinical and radiological features of ureteric dissection secondary to pelvic malignancy and to emphasize the critical importance of early diagnosis and timely management in preventing serious complications [2].
Ureteric dissection acts as a transient warning sign of an impending ureteric rupture. Dissection can lead to more severe complications if not promptly identified and addressed. Ureteric rupture can result in the leakage of urine into surrounding spaces, leading to severe conditions such as urinoma, which is a localized collection of urine that can cause abdominal pain and swelling. Additionally, the escape of urine into the perinephric or retroperitoneal spaces can result in the formation of abscesses, which may lead to infection and sepsis if left untreated [3].
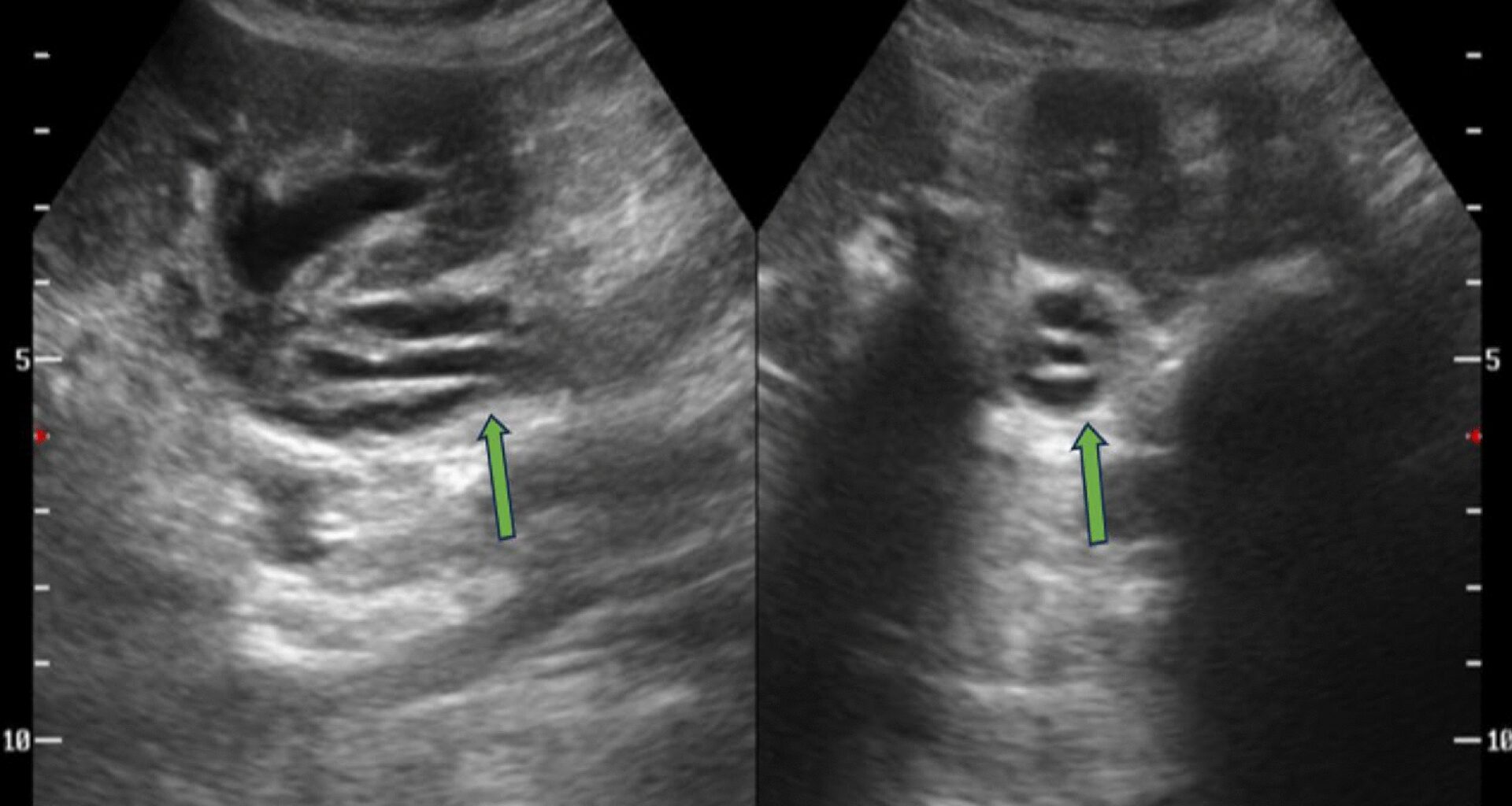
Imaging techniques play a pivotal role in the timely diagnosis of ureteric dissection. Contrast-enhanced computed tomography (CT) / CT urography and ultrasonography (USG) are instrumental in detecting the characteristic features of ureteric dissection and guiding appropriate clinical intervention. CT imaging provides detailed cross-sectional views that can reveal the extent of dissection and can also be used for interventions such as CT-guided aspiration. USG can be utilized for real-time assessment of the ureteral layers and surrounding structures [4]. The characteristic “double lumen sign” represents a thin hyperechoic linear echogenic strand on USG and a thin isodense-hyperdense linear structure seen on CT, representing medially displaced lamina by the collection of urine in between the mucosal and muscular layer, resulting in the formation of the two lumens, a true and a false one, similar to those seen in aortic dissection [5]. Timely diagnosis through these imaging modalities allows clinicians to implement strategies such as ureteral stenting or surgical repair, which are essential in preventing the progression from dissection to full-blown rupture.
A comprehensive PubMed review of the literature indicates that instances of ureteric dissection are exceedingly rare, with fewer than three documented cases in the medical literature. Xia et al. [5] reported two notable cases of ureteric dissection resulting from distal ureter ligation and external compression from rectal malignancy. Both cases demonstrated the ‘Double Lumen Sign,’ a radiological finding similar to that observed in vascular dissection, which was crucial for diagnosing ureteric dissection. The close differential is Ureteral double lumens, representing a rare form of ureteral duplication where the normal ureteral lumen is partially or completely divided into two channels but remains fused at the distal end of the split. It can be differentiated from dissection by appreciating the concentric medially displaced ureteric mucosal layer in contrast-enhanced CT [6]. These reports underscore the condition’s rarity and highlight the importance of recognizing the ‘Double Lumen Sign’ as a diagnostic clue for this severe complication.