
13 Mar 2026
Blood tests for Alzheimer’s disease are rapidly transforming the way clinicians diagnose the disease. Still, some scientists urge caution when interpreting results, arguing that the meaning of a positive blood test is not yet fully understood. Case in point: In the March 11 Nature Medicine online, scientists led by Mathias Jucker at the University of Tübingen, Germany, reported that people suffering from systemic amyloidoses have blood p-tau levels as high as those of AD patients.
In people with systemic amyloidoses, serum p-tau181 was as high as in AD patients.
Ditto for serum p-tau217.
Assays specific for brain-derived tau might be needed to rule out these diseases.
“These findings suggest that elevated serum p-tau levels are not specific to Alzheimer’s disease … [This] may complicate blood-based presymptomatic AD diagnosis,” the authors noted.
Systemic amyloidoses are relatively rare, with a few thousand new cases each year in the U.S., most occurring in older people. The two most common forms are immunoglobulin light chain amyloidosis (AL) and transthyretin amyloidosis (ATTR). In both cases, the affected protein misfolds into amyloid that deposits in the heart, kidneys, and peripheral nerves. AL and ATTR often damage the heart and/or cause polyneuropathy. To date, there are no definite blood-based biomarkers for these disorders.

Peripheral Amyloid Marker? Adjusted for age and sex, serum p-tau181 detects systemic immunoglobulin light chain amyloidosis (AL) and transthyretin amyloidosis (ATTR), but not polyneuropathy (PNP) from other causes. Stars indicate statistical significance. [Courtesy of Kaeser et al., Nature Medicine, 2026.]
Because amyloid deposits in the brain trigger nearby neurons to release p-tau, the authors wondered if peripheral amyloid would do the same thing. To investigate, joint first authors Stephan Kaeser and Anna Hofmann at Tübingen and Stephanie Schultz at Massachusetts General Hospital, Boston, analyzed 280 serum samples from four European sites. In total, they obtained 97 samples from people with AL, 52 from people with hereditary ATTR, and 30 from people with sporadic ATTR. The authors also analyzed 30 samples from people with a polyneuropathy not caused by amyloidosis, and 71 samples from healthy age-matched controls.
As predicted, people with AL or ATTR had higher serum p-tau181 than did controls, as measured on the Quanterix Simoa HD-X platform. The findings were statistically significant (image above). AL elevated p-tau181 more than did ATTR. In addition, for both diseases, p-tau181 tended to be higher if the person had polyneuropathy. This is likely because polyneuropathy indicates more advanced disease, the authors noted. In people with polyneuropathy not caused by amyloidosis, p-tau181 levels were the same as in controls.
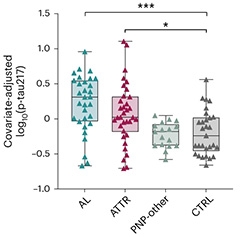
Not Just AD. Adjusted for age and sex, serum p-tau217 in AL and ATTR surpasses that in controls and other causes of polyneuropathy. Stars indicate statistical significance. [Courtesy of Kaeser et al., Nature Medicine, 2026.]
One of the cohorts, comprising 114 people from Heidelberg, Germany, included serum p-tau217 data. Again, as per Quanterix assay, p-tau217 levels were significantly higher in the 31 people with AL and 36 with ATTR, compared with 18 polyneuropathy patients and 29 controls (image at right). Curiously, p-tau217 better discriminated ATTR than did p-tau181. The latter marker was only elevated in ATTR patients with polyneuropathy, whereas p-tau217 rose even in those without it.
However, p-tau181 was a slightly better diagnostic overall, flagging systemic amyloidoses with an accuracy of 82 percent, compared with 77 percent for p-tau217. In addition to potentially helping diagnose AL and ATTR, these markers could help rule out those disorders in people with polyneuropathy, the authors suggested.
In both AL and ATTR, p-tau levels were about 2.5 times higher than in controls. This is similar to their elevation in AD, meaning clinicians would not be able to distinguish between peripheral and central amyloidosis based on a blood test alone. One way to tell them apart? Measure the size of p-tau fragments, because peripheral neurons make a larger version of the protein than do central ones. The field is already working on assays for the smaller “brain-derived” tau, and reporting superior performance (Aug 2025 conference news).—Madolyn Bowman Rogers
News Citations
Brain-Derived Versions of Phospho-Tau Make Better Markers 14 Aug 2025
Primary Papers
Kaeser SA, Schultz SA, Hofmann A, Häsler LM, Xu Y, Lambert M, Obermüller U, Brockmann K, Bijzet J, Nienhuis H, Nuvolone M, Obici L, Palladini G, Hegenbart U, Schönland SO, Jucker M.
Blood phosphorylated tau elevation as a biomarker in immunoglobulin light chain and transthyretin amyloidosis.
Nat Med. 2026 Mar 11; Epub 2026 Mar 11
PubMed.