
In this study, the authors examined various health and demographic indicators across Bangladesh and found regional disparities in maternal and child health outcomes. The country shows homogeneity in certain demographics, but significant regional differences exist in health-related measures. The literacy rate among young women (aged 15–24 years) in Bangladesh stands at 88.7%, which is almost similar to the South Asian average of 88.63%, but lower than the global figure of 90.93% according to World Bank Open data21. Although mobile phone ownership has significantly risen in recent decades, it still remains low among women in many developing countries, such as Bangladesh. A study revealed that women with higher socioeconomic status were more inclined to own mobile phones in the country22. Forty-five districts have been identified as having notably lower internet access at home and lower ownership of mobile phones among women aged 15 to 49 years, with divisional headquarters like Barisal, Khulna, Mymensingh, Rajshahi, Rangpur, and Sylhet. These findings are consistent with another study9. Rich or poor people, especially those living in rural areas, now have the opportunity to obtain medical advice thanks to mobile phone service. Whether it is late at night, a serious health issue, or a long way from the hospital, medical advice can now be obtained promptly. In cases where patients do not require hospitalization, they can receive guidance via a mobile device. Through the program, citizens may steer clear of unlicensed healers who could cause health problems. By doing this, the chance of disease complications is reduced23,24.
The World Health Organization (WHO) recommends early initiation of breastfeeding within the first hour after birth as a best practice. Globally, the rate of early initiation of breastfeeding is around 42%25. In European countries, this rate stands at 43%26, while in Asian countries, the prevalence falls between 38.7% and 42%27,28,29. Bangladesh performs better than the regional and global averages in early initiation of breastfeeding, with 46.6% of newborns breastfed within the first hour. The breastfeeding indicators show minimal variation across the country. This finding is supported by a prior study, which mentioned that breastfeeding prevalence differs by Bangladesh’s administrative divisions, with Khulna division having the lowest prevalence (51.71%) and Rangpur division having the highest (66.57%), followed by Sylhet division (66.13%)30. In total, 17 districts significantly lag behind the national average regarding the number of infants breastfed within one hour of birth. In contrast, the rate of feeding children aged 0–23 months with a bottle with a nipple is higher in these districts. At the same time, in these districts, the mothers of children aged 2–4 years are involved in four or more activities.
Literacy indicators show that ten districts, namely, Bandarban, Cox’s Bazar, Gazipur, Rajbari, Narail, Mymensingh, Joypurhat, Nilphamari, Habiganj, and Maulvibazar fall behind the national average. These districts must be improved to meet the national standards. Knowledge of HIV/AIDS is low among female adolescents, with only 11.6% having comprehensive knowledge, which is about half of the prevalence seen in India. A study reported that approximately 21.71% of women aged 15–19 and 25.38% of women aged 20–24 in India who are aware of HIV possess comprehensive knowledge about HIV/AIDS31. There is a significant discriminatory attitude towards people living with HIV in Bangladesh, with 44.7% 11. Notably, 34 districts have more discriminatory attitudes towards people living with HIV compared to the national average. These same districts also have lower levels of knowledge among women regarding where to get tested for HIV.
Reproductive health indicators are crucial for evaluating the state of maternal health in Bangladesh. Disparities are evident in antenatal care coverage, skilled attendants at delivery, institutional delivery practices, and cesarean delivery rates, post-natal health checks for newborns and mothers, with 29 districts falling below national averages32. These districts require enhancements to meet the national benchmarks. Institutional delivery rates have improved from 4 to 49% between 1993 and 201833, yet skilled birth attendants and facility-based deliveries remain lower than global averages. The global coverage of skilled attendants at childbirth increased from 62% in 2000 to 86% in 202334. However, Bangladesh lags significantly behind, with a national prevalence of 57%. Previous research has shown that the utilization of safe motherhood services, such as facility-based deliveries and skilled birth attendance, remains alarmingly low across Bangladesh, with certain regions exhibiting particularly dire statistics in this regard35. The percentage of women with Cesarean-section deliveries has continued to increase, from 3% in 1999–2000 to 9% in 2007, 17% in 2011, 23% in 2014, and 33% in 2017-1833. Cesarean delivery rates in Bangladesh exceed the WHO’s recommended target36, with a national average of 36% and even higher rates in the majority of districts, although the lower-performing districts have rates closer to the WHO benchmark. A study highlighted the regional variability of C-section deliveries in Bangladesh and mentioned that the prevalence of C-section deliveries varied in urban and rural areas of different divisions in Bangladesh, which is consistent with the findings of the study32.
Underweight prevalence, stunting prevalence, and wasting prevalence were higher in underperforming districts compared to national averages. In contrast, overweight prevalence was higher in the better-performing districts. This finding is consistent with a prior study9. Precious studies also showed that regional disparities are observed in the prevalence of stunting, wasting, and underweight among children in Bangladesh37,38,39,40,41. Socioeconomic factors like income, education, and access to health services were key determinants of these regional disparities9. Regional disparities are also evident among the districts in terms of the living in a safe and clean environment indicator. Disparities are evident in the use of improved drinking water sources, Handwashing facilities with water and soap, use of improved sanitation facilities, and Basic drinking water, sanitation, and hygiene services, with 10 districts falling far behind the national averages.
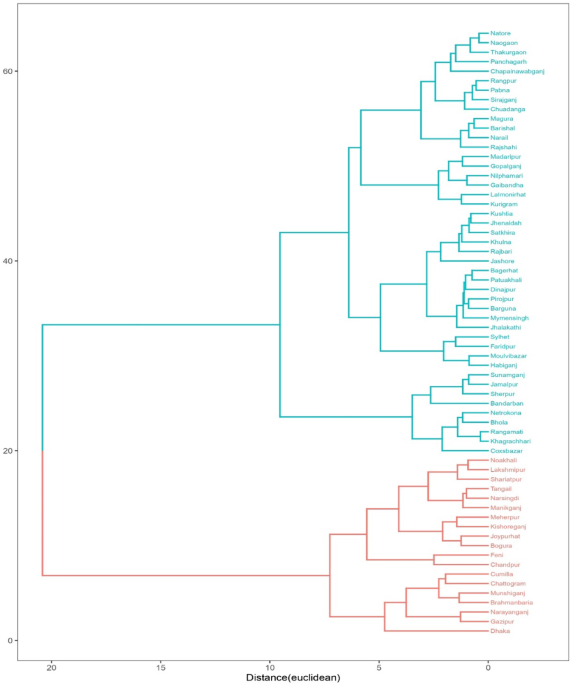
Based on the overall indicators, Bangladesh can be categorized into two separate clusters, containing 38 districts in one and 26 districts in the other. The underperforming districts are primarily located in the northern and northeastern regions, whereas the majority of the well-performing districts are situated in the central and southwestern areas of Bangladesh. The Chittagong Hill Tracts and certain southern districts are also categorized as poorly performing regions. These findings are supported by a previous study, and researchers pointed out that Bangladesh can be divided into two distinct clusters, with 35 and 29 districts in each cluster9. These findings suggest a need for region-specific interventions to address the health disparities. This includes improving accessibility and affordability of quality services in disadvantaged areas, implementing geospatial tools for monitoring, and designing targeted interventions. It also highlights the importance of increasing awareness among health service providers and households, as well as decentralizing health planning and budgeting to optimize health outcomes at the sub-national level. By applying cluster analysis to district-level maternal and child health (MCH) indicators, the study reveals distinct regional disparities that traditional national averages often obscure. These disparities suggest that a uniform approach to health intervention may be insufficient to address localized needs effectively. Districts identified in clusters with poor MCH outcomes require targeted, context-specific strategies, including improved healthcare infrastructure, increased availability of skilled birth attendants, and enhanced access to antenatal and postnatal care. Using cluster analysis, the study identifies groups of districts that share similar health challenges, allowing for more precise intervention planning. Instead of applying health policies nationwide, the findings advocate for region-specific strategies that address the unique needs of underserved districts. Furthermore, this data-driven approach can improve health equity and optimize resource use, offering policymakers a valuable tool for prioritizing areas with the greatest need.