
Currently, the treatment regimen for pancreatic tuberculosis, like that for abdominal tuberculosis, generally follows the protocols used for pulmonary TB [3]. Standard first-line ATT administered over 6–12 months demonstrates favorable outcomes in various studies. This case report marks the first documented use of RAI of isoniazid combined with oral antituberculosis medications for treating pancreatic tuberculosis.
RAI has not been utilized in previously reported cases. RAI therapy emerged in the 1960s, initially targeting severe acute pancreatitis and inoperable advanced tumors. The cytotoxic effects of the drug on tumor cells are concentration-dependent. The central principle of treatment is to achieve a localized high concentration of the drug through arterial infusion around the lesion, thereby maximizing therapeutic efficacy while minimizing collateral damage to unaffected organs.
The advantages of RAI are as follows [4, 5]:
1.
In intravenous administration, pancreatic blood flow constitutes only 0.8% of the total cardiac output, making it challenging for the pancreas to achieve an optimal therapeutic drug concentration after systemic administration.
2.
RAI involves the direct injection of drugs into the nutrient arteries supplying the diseased area of the pancreas. This method increases drug concentration in the region by 5 to 10 times compared to systemic intravenous administration, making RAI a potent approach for enhancing the treatment of severe acute pancreatitis and Pancreatic cancer from a pharmacokinetic perspective.
3.
RAI selectively or super-selectively delivers drugs directly into the nutrient arteries of the diseased pancreatic area, thereby circumventing the hepatic first-pass effect and allowing for a rapid and sustained increase in local drug concentration. Additionally, following arterial administration, the drug enters the liver through the portal vein, where it undergoes metabolism, potentially reducing systemic adverse effects.
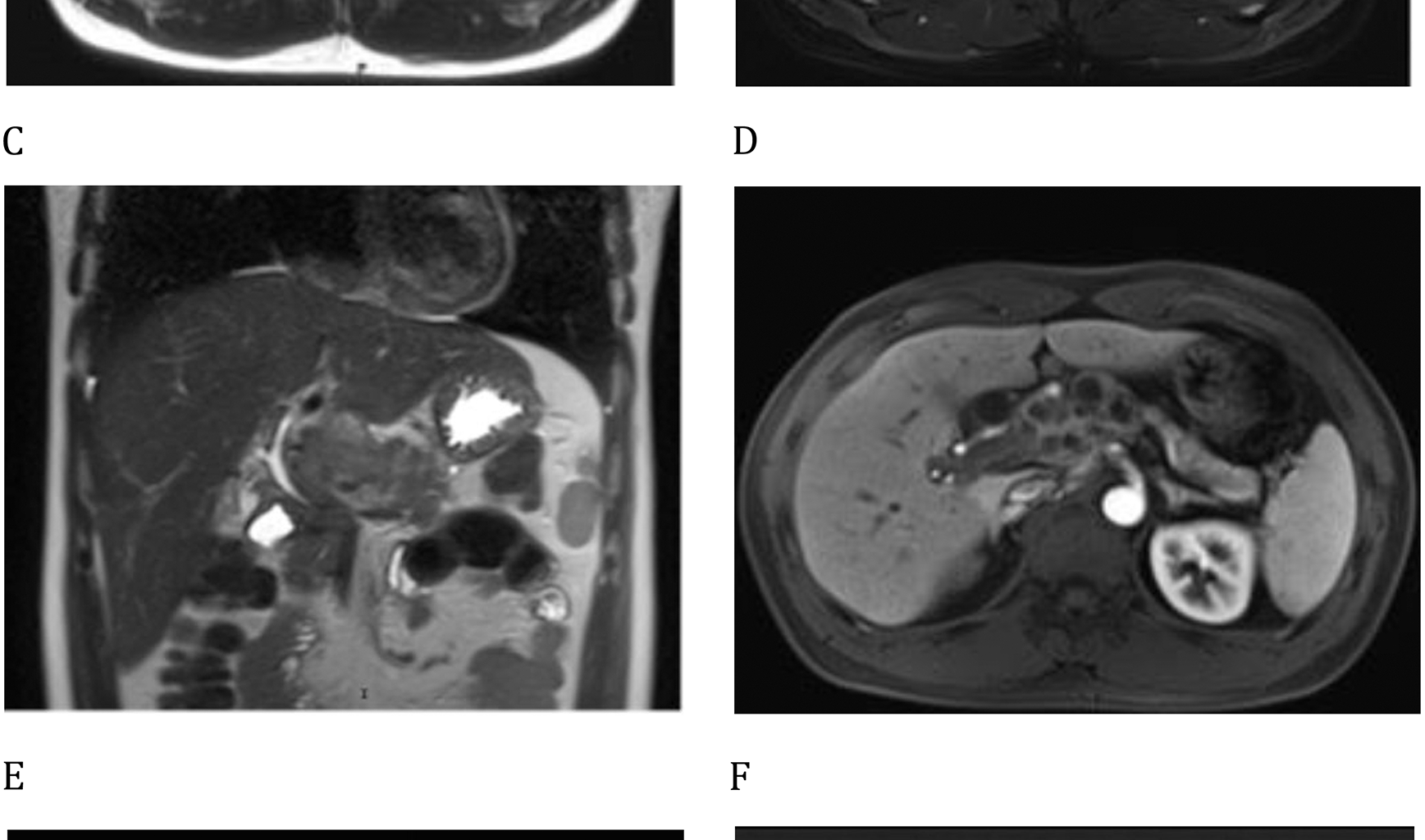
Tuberculous granulomas, the common form of tuberculous lesions, are typically composed of centrally located activated macrophages harboring tuberculosis bacteria, surrounded by peripheral lymphocytes and fibroblasts. After enhanced MRI analysis, the peripheral enhancement seen in these lesions highlights the distinct arterial blood supply to tuberculous granulomas, providing a theoretical basis for the use of RAI. Isoniazid is the first-line drug for the treatment of tuberculosis and is effective in managing both active tuberculosis and latent infections [6]. It is often used as a monotherapy or in combination with other agents. Isoniazid exhibits selective antibacterial activity against Mycobacterium species, likely due to its ability to inhibit the synthesis of mycolic acid, which is essential for the formation of the bacterial cell wall.
We administered a dose of 300 mg for arterial infusion in the patient, which corresponds to a single oral dose used in pharmacological treatment. Additionally, there is no cross-resistance between isoniazid and other anti-tuberculosis drugs, facilitating subsequent oral drug therapy for the patient. High-concentration isoniazid infusion therapy at the local site caused transient impairment of liver function in the patient. The AST and ALT levels declined below admission levels within one week.
In comparison with previous case reports and literature reviews, the 13-month total treatment duration in our case did not demonstrate significant temporal differences from conventional regimens. However, the rapid alleviation of the patient’s epigastric distension and pain through regional arterial infusion (RAI) therapy provided substantial clinical benefits during the initial treatment phase. This early symptom resolution markedly improved the patient’s quality of life and psychological distress at the critical onset period. While these observations are inherently limited by the single-case nature of this report, all therapeutic decisions were strictly guided by immediate clinical necessities, and the outcomes reflect objective treatment responses. Additional case series will be required to establish the long-term outcomes and safety of this therapeutic strategy.
Recent years have seen a gradual increase in case reports of pancreatic tuberculosis, yet comprehensive epidemiological data on its exact incidence remain incomplete. The occurrence of solitary pancreatic tuberculosis, as presented in this case, is an even rarer event. This rarity could be due to the antimycobacterial properties of pancreatic lipase and deoxyribonuclease [7]. Destructive lesions typically develop only after the inoculation of a significant quantity of Mycobacterium tuberculosis into the pancreatic parenchyma within a short period. The mechanisms by which Mycobacterium tuberculosis invades the pancreas are not well understood. Potential infection pathways include hematogenous and lymphatic dissemination from latent or secondary tuberculosis infections. Another possible route is from contiguous organ involvement, notably in cases of intestinal tuberculosis where TB originates from TB organisms within the liver and spreads via the biliary tract [8].
Clinical symptoms in patients with pancreatic tuberculosis are generally consistent, often beginning with acute or chronic abdominal pain and discomfort, which can lead to complications such as gastrointestinal bleeding [9] or acute/chronic pancreatitis [10]. An analysis of 166 cases of pancreatic tuberculosis showed a higher diagnosis rate among Asians [11, 12], with an average age of 41.6 ± 13.95 years and a male predominance, aligning with the demographic profile of the patient in this case. Among these patients, 25.3% were co-infected with HIV. Furthermore, the mortality rate among patients with confirmed pancreatic TB was 10.8% during hospitalization, with a follow-up mortality rate of 37.5% observed over a period ranging from 3 weeks to 32 months.
Pancreatic tuberculosis can occur in all anatomical regions of the pancreas, including the head and tail, with the pancreatic head being the most frequently involved site [13]. The lesions typically manifest as solid masses or cystic formations, often demonstrating radiographic calcifications. These pathological changes may cause compression or obstruction of adjacent vascular structures, including the portal vein, superior mesenteric vein, and hepatic artery [14]. During the initial imaging diagnosis, differential diagnosis between pancreatic tuberculosis and pancreatic cystic neoplasms must be carefully considered [15]. The laboratory indicators of pancreatic tuberculosis exhibit limited specificity. As an infectious pathology, pancreatic tuberculosis typically presents with an elevated erythrocyte sedimentation rate (ESR) and variations in blood parameters, which are potential markers for initially differentiating between pancreatic lesions and neoplastic processes. Pancreatic tuberculosis may also show elevated levels of tumor markers such as CA125 and CA199 [16, 17], as well as increased AFP levels, which could lead to a misdiagnosis as pancreatic cancer. The rise in CA199 levels has been linked to potential associations with pancreatic head masses and gallbladder obstruction caused by enlarged lymph nodes.
EUS-FNA has become an essential diagnostic tool for evaluating pancreatic and peripancreatic lesions, as well as for investigating abdominal masses and enlarged lymph nodes. When conventional acid-fast bacilli tests are negative despite clinical suspicion of tuberculosis, EUS-FNA should be considered as a diagnostic adjunct [18, 19].
In summary, isolated pancreatic tuberculosis represents a rare clinical entity. We have presented a comprehensive documentation of the diagnostic and therapeutic process in this case. The RAI therapy provided prompt resolution of the patient’s epigastric distension and pain symptoms, while subsequent combination with ATT demonstrated favorable therapeutic outcomes.