
The most effective vaccine program in American history doesn’t require a single new drug, clinical trial, or breakthrough. It requires a form for school enrollment.
But that’s changing. School vaccination requirements are being threatened from multiple angles: rhetoric from the highest offices of the nation is trickling down to state legislatures, and more people are having questions at kitchen tables and in pediatricians’ offices.
We asked for your questions. We have answers.
School and childcare vaccine requirements have always lived at the state level. For most of modern history, that didn’t matter much. All 50 states landed roughly in the same place: protect kids from measles, polio, chickenpox, and hepatitis B. Every state also has medical exemptions (a doctor confirms the vaccine isn’t safe for a specific child). The majority of states have non-medical exemptions (religious, philosophical, or personal belief).
But things are shifting.
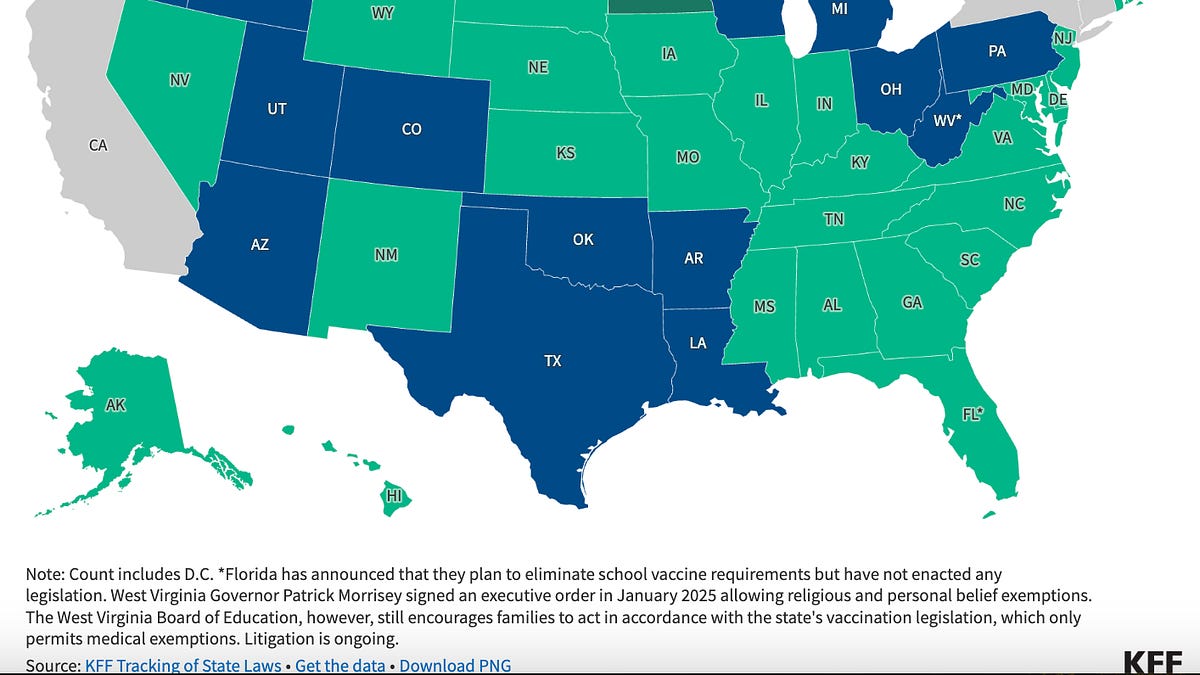
The strictest states may be becoming more lenient. Five states—California, New York, Maine, Connecticut, and West Virginia—allow only medical exemptions. And this is fairly new. That’s now under legal pressure, including a Supreme Court case expected this summer and active debates in West Virginia.
On the other hand, states that were already lenient are looking to become more so. More than 200 bills are being introduced about vaccines, including school requirements:
In 2025, Idaho passed a “medical freedom” law that bars schools from conditioning enrollment on vaccination, making its existing requirements challenging to enforce.
Ten other states passed legislation or took administrative action to weaken or eliminate requirements. Iowa and Florida have seen the most serious pushes, though Florida’s most aggressive proposals stalled this cycle.
Our read: this debate will largely stay at the margins. Three out of four Americans still support school vaccination requirements, including two-thirds of Republicans. But the pressure is real and worth watching.
Yes, but the reason might surprise you. Most people assume the logic is simple: you have to vaccinate to enroll, so you do. But the evidence points to something more interesting.
Requirements work in part by creating a structured moment of connection to health care, which is often a catch-up opportunity for overdue preventive care. They remove the friction that keeps well-meaning families from staying up to date. That mechanism has real implications for what’s lost when requirements are removed.
Several findings support this:
When families do come in to meet school requirements, they don’t just get the required vaccines. Requirements increase uptake of non-required vaccines like HPV, too.
The biggest gains show up among children who were simply behind, not among children of vaccine-refusing parents.
When states eliminate non-medical exemptions, families seeking medical workarounds barely budge (rising only about 0.4 percentage points).
Some Canadian provinces and the U.K. achieve comparable vaccination rates without requiring school entry by delivering vaccines directly in schools.
This health care connection matters far beyond vaccines. Developmental delays, lead exposure, vision problems, food insecurity, and signs of abuse are all routinely caught at these same visits. Weakening requirements doesn’t just lower vaccination rates but also cuts off one of the few reliable ways for children to connect with a doctor.
That said, requirements are only as equitable as the system behind them. In a 2024 survey, almost 1 in 4 parents who sought an exemption cited logistics, not philosophy, as the barrier. That’s an argument for pairing requirements with robust access.
It depends on the disease we are talking about. Vaccines do not all work the same way. Some, like measles, are extraordinarily effective at preventing infection, while others are meant to protect from severe illness, and many have protection that wanes over time.
For measles, the MMR vaccine is insanely effective (97% effective after two doses). But a few nuances matter:
Disruption. When measles enters a school, protocols require unvaccinated students and staff to be excluded for up to 21 days per exposure. Your vaccinated child may be fully protected, but still caught in weeks of school disruption.
Who’s at home? Vaccinated individuals can carry the virus before their immune system clears it. If you have an infant too young to be vaccinated (MMR starts at 12 months) or an immunocompromised family member, a school outbreak can reach your home.
Vaccine non-response. About 3–5% of people don’t develop full immunity after the MMR vaccine. You can check your antibody levels with a titer test, but even that doesn’t tell the complete story.
For diseases like whooping cough or mumps, the concern is different. The vaccines work well at preventing serious illness, but they’re not as effective at stopping the spread of disease. This means even vaccinated people can sometimes transmit these diseases without realizing it.
High vaccination rates in your community protect everyone, including the small percentage of vaccinated people whose immunity didn’t fully take.
Yes. Several countries have already gone through versions of this debate, and their experiences reveal a few consistent patterns worth understanding.
Italy’s story is possibly the most instructive. Italy had requirements on the books for decades, but rarely enforced them. A 2012 court ruling falsely linking MMR to autism went viral, and coverage collapsed. A 2017 outbreak with 5,000 measles cases and four deaths led to stricter requirements. However, the hard mandates also triggered fierce public backlash, giving the incoming populist government the political opening to weaken it almost immediately. Measles surged again. Italy has since reinstated stronger requirements, but the cycle illustrates two lessons: rollbacks will cause outbreaks, and how you implement requirements may shape whether they survive the next election.
How you talk about this matters just as much as what you say. The right approach also depends on who you’re talking to.
Don’t lead with science and data. When people feel like their values are being challenged, facts alone rarely change minds. Start with shared values, then let the evidence support the conversation.
Begin with common ground. Most parents, regardless of their politics, want their kids to be safe at school and for school to run normally. Saying “I just want to make sure schools aren’t shut down for weeks because of a preventable outbreak” is something almost everyone can agree with. Start there.
If someone brings up studies or claims that seem to contradict the evidence, resist the urge to debate every detail. Instead, acknowledge the concern and emphasize that what matters most is the totality of the evidence.
Words matter. Avoid the word “mandate.” It tends to put people on the defensive immediately. Try “school immunization requirements” instead, and use “immunizations” rather than “vaccines” to sidestep some of the charged associations from COVID-19 debates. This framing also helps because school immunization requirements are just one part of standard enrollment paperwork, like getting a vision screening or a physical. Framing it that way makes it feel less like a political battle and more like a routine part of keeping kids healthy.
For policymakers, the financial argument is often the most persuasive when other arguments stall. The 2019 measles outbreak in New York cost over $8 million to contain. Requirements are cheap, and outbreaks are expensive.
It’s also worth emphasizing that there’s a range of middle-ground options that don’t require choosing between eliminating requirements entirely and keeping them exactly as they are. Policymakers can make exemptions harder to obtain without eliminating them, require families to complete vaccine education before receiving an exemption, or restrict exemptions on a disease-by-disease basis rather than all at once. As Italy showed, going too far too fast can turn supporters into opponents. The goal is durable policy, not just bold policy.
School vaccine requirements do important, quiet work: they keep preventable outbreaks out of classrooms, keep kids in school, and create reliable moments for families to access health care they might not otherwise get. Three out of four Americans support keeping these requirements. The challenge now is to make sure the majority is heard.
Love, YLE and DH
David Higgins, MD, MPH, is a practicing pediatrician and public health physician whose work focuses on vaccine delivery, health policy, and communication. He publishes the newsletter Community Immunity, where he writes about vaccines and public health. When he’s not seeing patients or writing, he’s coaching youth soccer or exploring the outdoors with his family. Find him on LinkedIn and Instagram.
Your Local Epidemiologist (YLE) is founded and operated by Dr. Katelyn Jetelina, MPH PhD—an epidemiologist, wife, and mom of two little girls. YLE reaches more than 425,000 people in over 132 countries with one goal: “Translate” the ever-evolving public health science so that people will be well-equipped to make evidence-based decisions. This newsletter is free to everyone, thanks to the generous support of fellow YLE community members. To support the effort, subscribe or upgrade below: