

Characteristics of participants
A total of 43 individuals participated in the FDGs – 25 women and 18 men. Of these, 32 had been born and raised in Jamestown/Usshertown, and the other 11 participants had been born outside these two communities but had lived in the study communities for more than 20 years. Most participants (n = 17) were < 35 years of age at the time of data collection, and ten were between the ages of 56 and 65 years. A high number of participants (n = 16) had attained secondary education. The remainder had attained primary education. Only a small number (n = 4) had attained tertiary education. Only three people worked in the formal sector; three participants were students, and the rest were employed in the informal sector, mainly as traders and fisherfolk. See Appendix 1 for full demographic details for all participants.
Several thematic areas dominated both the CM-FGDs and the trader FGDs. Key areas included lay perspectives of the community, descriptions of the built environment, environmental stressors, the food environment, and the perceived risk of diabetes and CVDs. A comprehensive thematic table showing all the themes and codes is attached as supplementary material. Figures 1, 2, 4 and 6 accurately represent the environment generated using QGIS to provide context to the qualitative discussions. Figures 3 and 5 are sample CMs produced freehand by community members.
Fig. 1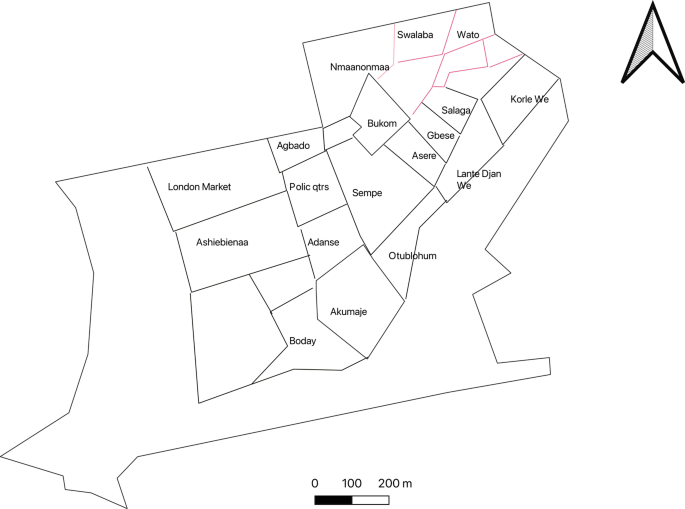
Community neighbourhoods in Jamestown and Usshertown. Source: Care Diabetes map, 2023
Fig. 2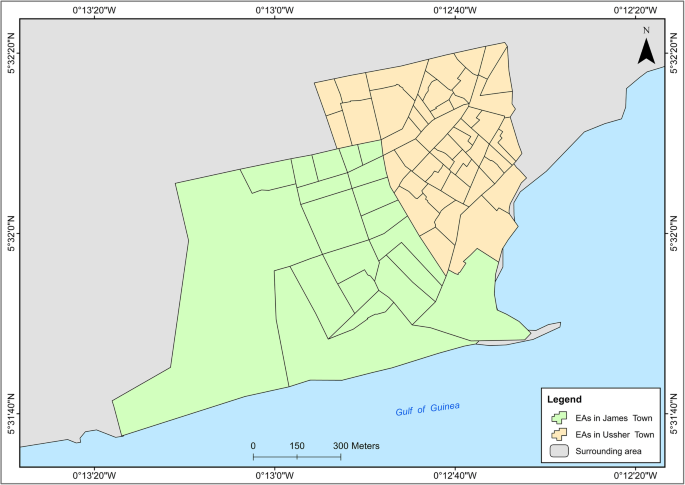
Administrative demarcation of Jamestown and Usshertown
Fig. 3
Sketch depicting connectivity in Jamestown. Map produced by woman from Jamestown
Perceptions of the definition of a community
Participants reported that a community is based on the built environment, ethnicity/clans, history and social behaviour. They emphasised that individuals must share community traits such as language and food to be seen as a community.
“A community is a group of people who may be many or not depending on the piece of land they have. They may be 1,000 or less than 1,000; it is a community. You can identify them with characteristics like their language, food and way of doing things. With my community, for example, you can identify us with our way of life, the way we dress, the food we eat among others.” Woman from Jamestown, FGD 4.
“As far as you can be found in one geographical area, and say that you recognize these people with these traits, it is definitely a community.” Man from Usshertown, FGD 4.
Participants noted that the two study communities (Jamestown and Usshertown) comprise people of the Ga ethnic group with different historical experiences. Participants referred to Jamestown as Ngleshie, British Accra; and Usshertown as Dutch Accra. They further subdivided Jamestown and Usshertown into clan units, clustered in specific locations of both communities. Sometimes, the community was defined in terms of these subdivisions. Participants mentioned the Akumaje, Sempe, Gbese, Otublohum, Asere and Abola clans. Sometimes, certain behaviours and practices were associated with these clan units.
“Where you [addressing another participant] live, we call that whole area, Akumaje.” Woman from Jamestown, FGD 2.
Descriptions of the built environment of Ga Mashie
Participants described the built environment according to neighbourhoods, connectivity, population density and the food environment. They deployed paths, edges, districts and nodes to explore the characteristics of the community.
Neighbourhoods in Ga Mashie
Participants used edges to indicate the boundaries of the neighbourhoods. Paths were used to show the street and road networks in the community. Nodes were used to show bus stops. Finally, boundaries were used to identify the geographic boundaries of the clan units within both communities. Figure 1 is an approximation of the neighbourhoods that was generated by the research team. During the daily debriefing sessions, the team developed a map to show the neighbourhoods that had been mentioned by community members. The community map in Fig. 1 differs substantially from the official map of Jamestown and Usshertown in Fig. 2. Figure 1 has 29 areas, while Fig. 2 has 82. Also, the Enumeration Area (EA) boundaries in Fig. 2 have no real meaning to the community. Community members did not use any known landmark to define community.
Connectivity or paths in Ga Mashie
Figure 3 is a sample map showing a participant’s perceived connectivity of Jamestown and Usshertown. Figure 4 is the GIS-generated map. While Figs. 3 and 4 look aesthetically different, they convey the same message that the community is interconnected to a high degree. The maps display the main roads, community vehicular routes and footpaths. There are 11 bus (trotro) stations in the communities. The dominant vehicles in the community are commercial motor bicycles, tricycles and minivans. Most Jamestown and Usshertown alleys are paved. This makes the roads and the interconnections accessible at any time, under any weather conditions. Participants reported that, before the pavements were laid, the community experienced flooding whenever it rained.
Fig. 4
Interconnectivity maps generated with GIS by the research team
Population density in Ga Mashie
The communities were described as overcrowded due to the density of people seen on the streets, in houses and in sleeping rooms. The residential blocks are large structures consisting of several single rooms. These structures are usually family houses that are shared by extended families across three to five generations. A household (on average, three members) often inhabits a single room and sometimes shares the space with an extended family member. The quotes illustrate these characteristics.
“Our household is in a family house. I have been given [one] room that I stay in, but because my sister has not been given hers, I share it with her and also with her children.” Woman from Usshertown, FGD 4.
“I live in [one] room with my husband, and we have four children who are not married; we all live there and that increases our population.” Woman from Jamestown, FGD 5.
Social spaces of Ga Mashie
Social spaces refer to places or centres where people gather and interact. Participants mentioned spaces such as pubs (‘drinking spots’), cinemas and ‘parliaments’ (Figures 5 and 6). They also mentioned social events such as funerals and naming ceremonies. These temporary spaces could be set up anywhere in the community, including in streets, courtyards and car parks.
Fig. 5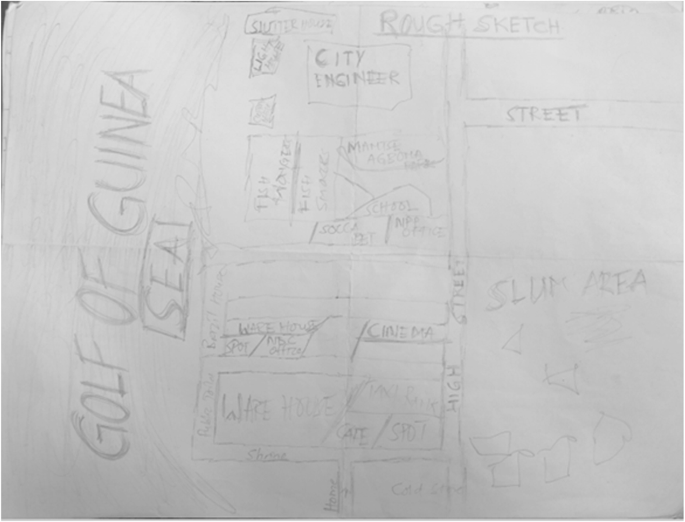
Cognitive map showing social spaces in the study communities
Fig. 6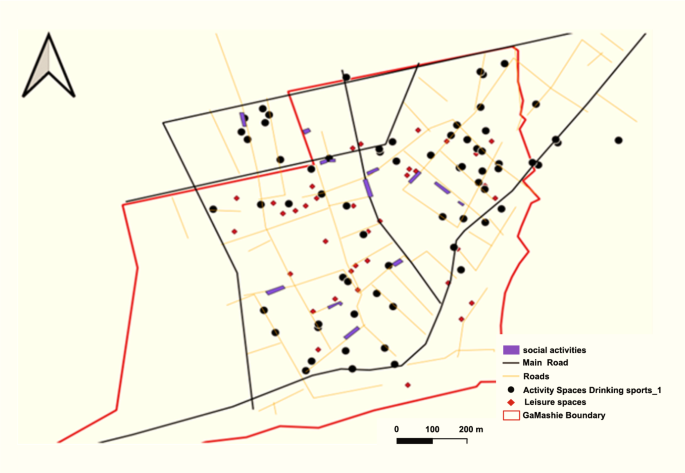
GIS-generated map showing social spaces in the community. Source: Care diabetes project, A social map of Jamestown and Usshertown
Figure 5 depicts a CM drawn by a respondent that shows two drinking spots, a café, a soccer betting shop, a warehouse, political party offices and other spaces. The only social space that appears twice on the same map is the drinking spot, emphasising its abundance in the community. The map also indicates the offices of the dominant political parties in Ghana (i.e., the New Patriotic Party (NPP) and National Demographic Congress (NDC)). These are sheds that are funded by the two parties where people sit and mingle. These spaces are often draped in the paraphernalia of political parties. Sometimes, local community members called these spaces ‘parliament’. Participants reported that there was limited activity within these spaces during the day. They came alive in the evenings when people returned from work and were available to socialise. Participants observed that men and male activity dominate these social spaces.
“With this parliament thing we are talking about, we have boys–boys joint, normal community groups joint, then we have the political joint like the NPP, NDC and CPP joints. Looking at the NPP joint, the people who sit there are big men not in the sense of the job they do but they have political influence. Because of the political influence they wield, they just sit there and get some stipends from the political leaders and come and share it. They will be sitting there and political leader will probably come and give them let say 100 cedis [US$8] to share. They go and sit there and maybe there is a political … even that is going to come on, if there is a job opportunity, they will be like ‘oh, we know this person because he has been coming to sit here with us so give it to him’. These are some of the benefits these people get by going to sit there.” Woman from Usshertown, FGD 5
The map depicted in Figure 6 is saturated with community leisure spaces and drinking spots. The study mapped 37 leisure spaces and 67 drinking spots in the two communities. Participants reported that almost all funerals occurred on community vehicular roads, which limits mobility.
“As for weddings, you hear of it once in a while. Funerals happen often and during funerals we drink and eat.” Woman from Usshertown, FGD 4
“Yes, after the rituals, you see, we have some two to three hours to have fun. That is where you see people smoking, mixing [alcoholic cocktails. That happens on the first day of the funeral. On the first [day] of the funeral, there is a lot of drinking and eating.” Man from Usshertown, FGD 4
Environmental stressors of the built environment of Ga Mashie
Participants described two significant environmental hazards due to overcrowding: hazardous heat and sound.
Hazardous community heat
Participants expressed strong opinions concerning heat intensity in the communities and how that affected their health. Heat, together with environmental stressors, was mentioned 35 times in the FGDs. Participants attributed heat in the community to population density, the built environment and related human activities, with population density cited most frequently (n=8). Other causes of heat included the spatial organisation of the neighbourhood, domestic and industrial cooking, the presence of a slaughterhouse, climate change and the weather. The effects of heat in the community included sleeplessness, mental health conditions, skin rashes and sleeping outside. Participants reported that heat drove people outdoors, and that heat from room overcrowding kept community members outdoors most of the day.
“Your aunt could light the coal pot to cook something. She cannot place it in the sun, so she will place it in front of you so we can both sit there. The fresh air cannot come through because the fire is in the way, so we are all experiencing the heat.” Woman from Usshertown, FGD 1
“From here to the house, there is a lot of heat and when you get home, the house is hot. Where will you go to?” Woman from Jamestown, FGD 2
Hazardous community noise
Hazardous noise was mentioned most frequently by participants as an environmental stressor. Overall, hazardous noise was associated with 83 different themes: primarily behavioural factors such as shouting, religious activities, industrial activities; vehicular activities, social activities such as funerals and naming ceremonies, sporting activities, alcohol vendors who play loud music all the time, and even family fights. Participants raised concerns about excessive and unregulated noise pollution at all times that pose a potential health and safety risk. Some participants shared their sense of powerlessness in response to the high volume and intensity of noise within the neighbourhood.
“As for the churches, I wouldn’t want to mention them because they will say I don’t like God. Regarding the churches, all-night programmes used to be only Fridays but now they do it Wednesdays and Fridays. So just imagine if you live closer to a church. We are becoming used to it because we have lived with it for quite some time. Also, they are playing their stuffs it vibrates a lot. As for the funeral, there are those who close theirs early but others will not. So how can you sleep on Sunday and go to work on Monday if you work? Some of them intentionally do the funeral for Lengthy hours to show off. But when I was growing up, it was not like that. Funerals used to close at around 5pm, and during the wake that music is played in the evening. But now there has been a lot of changes in that aspect.” Man from Usshertown, FGD 6
Noise, poor sleep, headaches, increased blood pressure
Participants believed that noise negatively affected several aspects of the community. They associated hazardous noise with a lack of peace of mind, leading to personal discomfort and psychological distress. This theme was recorded seven times in the FGDs and was only mentioned in reference to noise. Study participants linked noise intensity to headaches and a host of CVDs, including hypertension, chest pains and heart attacks. The quote below shows how community members link mental health stressors to heart health.
“When I sit down and you are standing close to me, making noise, I feel like I have a headache. It feels like you are exerting some pressure. It is like in my mind, there is a lot of noise, and I feel disturbed.” Woman from Usshertown, FGD 2
“It also brings about a headache, and sometimes you become startled as a result of the noise, and that can result in a heart attack. When someone shouts so loud, there can even be a rise in your blood pressure, which can create problems.” Woman from Jamestown, FGD 6
The street food environment in Ga Mashie
Food is a major aspect of community life. Participants described food availability, consumption time and taste as the main drivers of the changes in food culture. Participants noted that strong tastes drove the food culture, influencing food preparation. They noted the increased use of processed condiments and artificial flavouring (e.g. A1, Maggi), which were foreign to traditional food preparation methods. According to community members, using these condiments has shifted demand towards “tasty food” that has a “delicious taste”, which they associated with lifestyle diseases like diabetes. Street food vendors constituted the main food outlets in the community, selling ready-to-eat meals such as jollof rice, noodles, bread and kenkey (a popular fermented maize mixture with dough moulded into balls in a corn husk). Community members discussed the changes in the food culture, specifically the emergence and dominance of fried foods.
“Maggi, A1 and different spices. They use it to prepare the food just to make it taste good, but it is not good for our health.” Food vendor from Jamestown, FGD 8
Increased consumption of artificial seasoning
Participants reported that competition among street food vendors influenced the use of harmful cooking practices. Food vendors, however, argued that they only cooked according to the tastes of community members. Food vendors suggested that cooking practices adopted for commercial purposes differ from those used for domestic purposes. This highlights awareness of the risk associated with using strong, artificial flavours.
Many community members mentioned preferences for street foods as a notable risk factor for the rise in CVDs.
“Also, we use Maggi in almost all the food we prepare recently, which wasn’t like that in the olden days.” Food vendor from Jamestown market, FGD 7
“If the food isn’t tasty, they won’t buy, so the onus lies on you to make it tasty. Hence, Maggi must be used to get the desired taste.”Food vendor from Jamestown, FGD 8
Increased consumption of out-of-home meals
The high population density and lack of cooking units were cited as key factors associated with purchasing and consuming meals prepared outside of the home (‘out-of-home’ meals). Participants explained that there was some family pressure to share home-cooked food. Because living spaces are often small, overcrowded, and poorly ventilated, cooking typically occurs in courtyards. In these shared spaces, other family members may join in, and participants are often expected to share meals with their extended relatives. These conditions were viewed as obstacles to home cooking, making it costly and inconvenient, leading to greater reliance on food prepared outside the home.
“Currently, things are expensive in the world, and also people don’t get enough money for upkeep; cooking has become quite difficult. So people intentionally play with your kids so that you give them some after cooking, that’s when they realise that you are cooking.” Food vendor from Usshertown, FGD 8
Late-night meals
The risks related to food were due not only to cooking practices and taste, but also to the time that food is consumed. Participants noted that the communities were very vibrant at night and many social events continued late into the night. They saw eating late as a community behaviour associated with the risk of diabetes.
“When I eat late, I suffer from heartburn, and I also learnt that eating late raises one’s sugar level, which leads to diabetes. Also, you don’t have enough rest.” Man from Jamestown, FGD 6
Low physical activity
Low physical activity and limited opportunities for physical activity were cited frequently in the CM-FGDs. Participants observed that the communities’ parks, gyms and fitness centres only served younger male adults. There were generally not enough opportunities for women and older people to undertake physical activities. Even the pavements were occupied with street food, limiting walking and movement.
“Yes. At the roundabout there is space. They call the place Buduemu. You can exercise there but you need to pay for the place before you get to [exercise]. But at the roundabout, you will see only boys.” Woman from Usshertown, FGD1
Diabetes was mentioned eight times, with all occurrences associated with the social environment and lifestyle choices.
“I think we have hypertension resulting from too much fat, and then diabetes as a result of the sugary stuff like drinks.” Woman from Jamestown, FGD 2
“It’s like kenkey contains sugar, so when you over eat it, you may end up with diabetes.” Food vendor, Usshertown FGD 8
“Yes, when you realise what the customer wants, you do it for them. So if you go to the market and buy something else, you destroy your own market.” Food vendor from Jamestown FGD 8
“The food vendors prepare the food with a profit-making mindset. So they use much oil, Maggi and beef, but she prefers dried fish. So the food vendors use the beef and all those ingredients to make the food attractive and tasty. But that is what makes us sick but we have no idea.” Man from Jamestown, FGD5
“I think there is a shift in taste.” Man from Usshertown, FGD 4
Discussion
Communities thrive in spaces where people feel safe and valued. In turn, environmental harmony creates the safety and security needed to maintain optimal health [43]. Unfortunately, overcrowding and unregulated use of space generate stress and increase the risk of lifestyle diseases [43]. This is amplified by poorly designed cities [38, 44, 45] – which create environments where excessive noise, traffic, fear of crime and poor air quality represent risk factors for obesity and other CVDs [46].
This study documents community perspectives on the effects of a hostile environment on health in urban Accra. Community members believed that the physical environment and social factors contribute to the development of diabetes and CVDs. These risk factors were identified at the individual, household and community levels.
Risk factors are woven into community behaviour patterns through numerous platforms and community engagements. Notable diabetes and CVD risk factors, such as alcohol consumption, form an integral part of community life, for example at funerals. While acknowledging the history and culture of the community, participants also noted changing dietary patterns and lifestyles that increase the risk of diabetes and CVDs. Conversations predominantly focused on how changing food practices and behaviours contribute to risk factors associated with diet.
The community’s complex perspectives on the built environment highlight the challenges in scientific conceptualisation, measurement and understanding of the built environment and related risk factors. This may partly explain why a simple physical count of liquor outlets, parks, walkways and other environmental measures may not always directly predict the influence of the environment on CVD risks [47].
Previous studies have established the relationship between the built social environment and the risk of diabetes [48]. Ecological models emphasise the influence on behaviour at the level of the individual, group, community, built environment and social environment [9]. Many studies show that physical inactivity and the food environment are key risk factors for diabetes [48]. The built environment influences the risk and management of diabetes through the creation and availability of walkways, gyms and parks, and the concentration of food outlets. For example, the concentration of fast-food outlets in the UK is significantly associated with diabetes risk [49]. Within the social environment, hazardous noise is known to elevate stress levels and sleeplessness, and this has been associated with the risk of some CVDs and diabetes [50]. Participants made these associations to explain the risk of diabetes and CVD within urban Accra. These local understandings of the built environment provide an opportunity to engage community members and prescribe meaningful solutions.
Community heat and noise are noteworthy themes under which participants expressed powerlessness: people felt the impact of these environmental characteristics was beyond their control. The built environment and intense human activity produced a challenging environment in the study communities. People lived in multigenerational households, sometimes owned by whole clan units. No single individual necessarily had control over what occurred in these dwellings. However, the shared spaces offered some advantages too, such as giving people somewhere to reside for free in increasingly expensive urban Accra. The disadvantage is that community members do not choose the people they must live with, and they must do so indefinitely. Sometimes, several adult siblings shared a single room with their children because they inherited that space from a parent and therefore had an equal stake. In several other studies, powerlessness is associated with difficult inner-city neighbourhoods and is attributed to crime, violence and instability [51, 52]. In this study, however, participants associated powerlessness with the regular functioning of their community regarding noise, heat and even food. Participants’ inability to control the number of food outlets in their community and the processed goods available resulted in a harmful food environment that increased their risks of diabetes and other CVDs.
Lack of autonomy over their dwellings and other spaces within their community fuelled the perspective that elements within the environment cannot be controlled, even if the community had created those spaces. However, participants cited several examples where they could assert some control over community-level problems. For example, once every year, the community bans drumming and noise-making for a whole month preceding the annual festival. These bans are upheld with religious verve. Similarly, to control the noise level in neighbouring areas, some communities permit funerals only once per month rather than occurring at any time. This same energy could be channelled into managing other community-level phenomena that affect the health of large groups.
While there may be differences in context, it is noteworthy that community-level strategies have been proven to work in communities not far from Jamestown and Usshertown. Several active community organisations, such as market women’s groups, fishermen’s groups, youth groups and others, could be sensitised to advocate for community-level reforms through the traditional council and the Accra Metropolitan Assembly (AMA). Indeed, GAMADA exists for such a purpose, and it has successfully led several community-level initiatives.
Strengths and limitations
Using multiple methods allows one to observe the environment from various perspectives; however, synthesising observations from multiple perspectives can be challenging. As the study communities are multicultural, different language competencies were required to communicate effectively with participants. It was initially quite challenging to ask older community members with limited formal education to draw, but they eventually enjoyed the process.
While findings from this research may have implications for similar urban poor contexts in Ghana and beyond, the study was not intended to generalise the findings. The aim was to understand nuanced community perspectives on how the environment may influence the risks for diabetes and CVDs.