
Incidence burden of myocarditis from 1990 to 2019
Globally, the incidence of myocarditis was 1.27 million (95% UI = 1.02 to 1.53) in 2019, with a 62.2% increase from 0.78 million (95% UI = 0.62 to 0.95) in 1990. However, the global ASIR declined from 16.74 per 100,000 population in 1990 to 16.00 per 100,000 population in 2019 (Table 1).
Table 1 Incidence cases and ASIRs of myocarditis by SDI region, sex, and region in 1990 and 2019 and its EAPCs from 1990 to 2019
The EAPC represents the tendency of the ASIR (Table 1). The ASIRs decreased in the vast majority of regions between 1990 and 2019, with the largest decreases in America (EAPC= −0.83, 95% CI= −1 to −0.66) and the greatest increases in North Africa and Middle East (EAPC = 0.02, 95% CI = 0.02 to 0.02) and Eastern Europe (EAPC = 0.02, 95% CI = 0.01 to 0.02). However, no significant changes were detected in resting regions, including Southeast Asia, Oceania, the Caribbean, Central Europe, and southern sub-Saharan Africa, where the ASIR of myocarditis did not significantly change (all EAPC = 0) (Table 1).
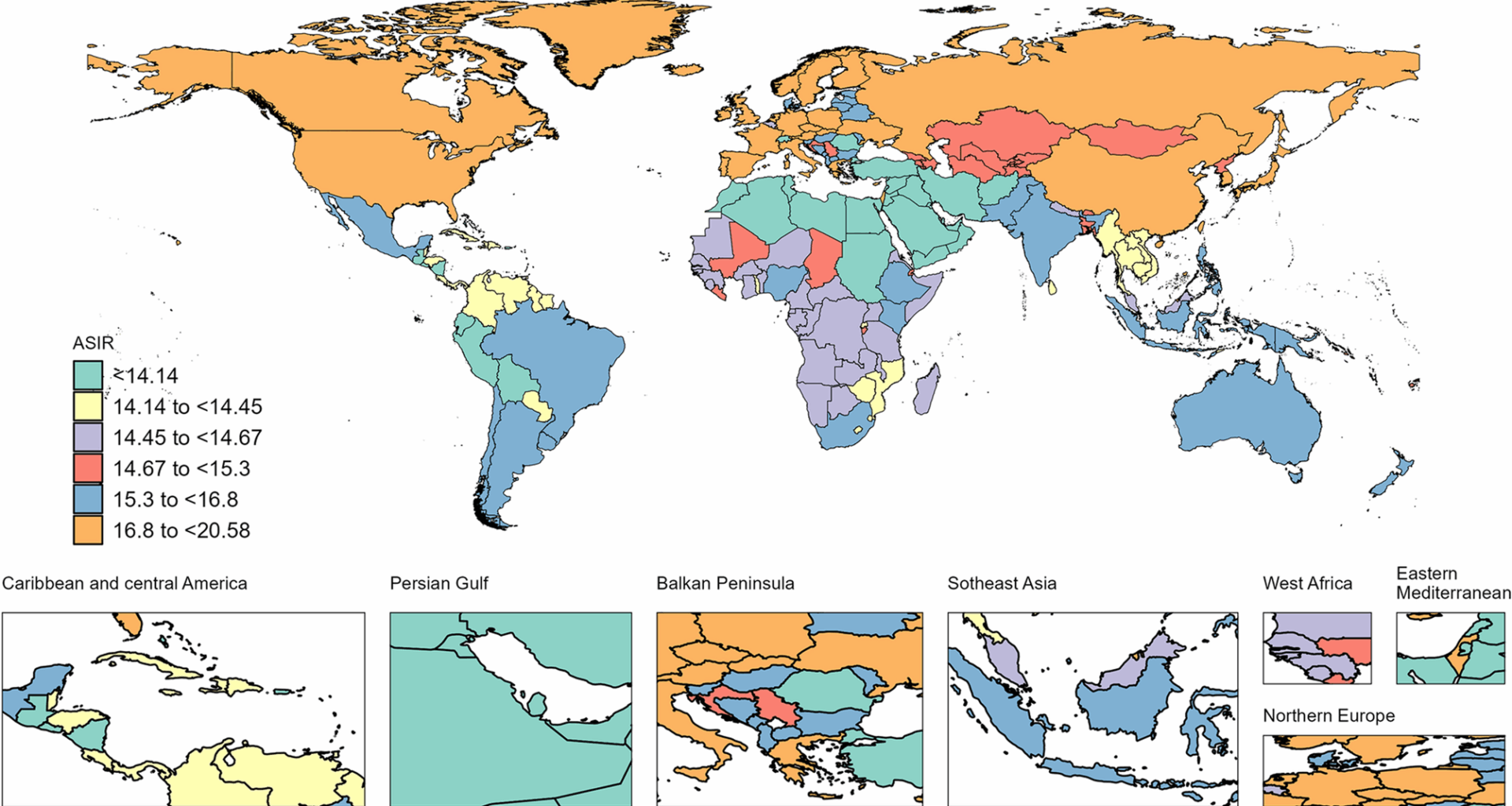
Regionally, for the ASIRs of both sexes, Japan, Austria, and Sweden presented the highest ASIRs in 2019, whereas Lebanon, Palestine, and Tunisia presented the lowest ASIRs at the same time (Fig. 1). From 1990 to 2019, the ASIRs in the global, high-SDI, high-middle-SDI, and middle-SDI regions decreased. However, the ASIRs in the low-SDI and low-middle-SDI groups remained stable. The highest and lowest ASIRs were associated with high SDIs and low SDIs, respectively (Fig. 2A). Countries with a high SDI had a faster decrease in ASIR than did those with a low SDI, with average annual percent changes of −0.01% (95% CI= −0.02% to −0.01%) and − 0.2% (95% CI= −0.26% to −0.15%), respectively (Fig. S1A).
Fig. 1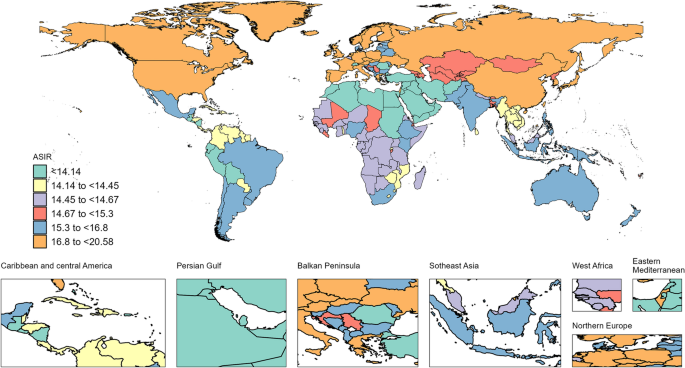
ASIRs of myocarditis in 204 countries and territories in 2019. ASIR, age-standardized incidence rate
Fig. 2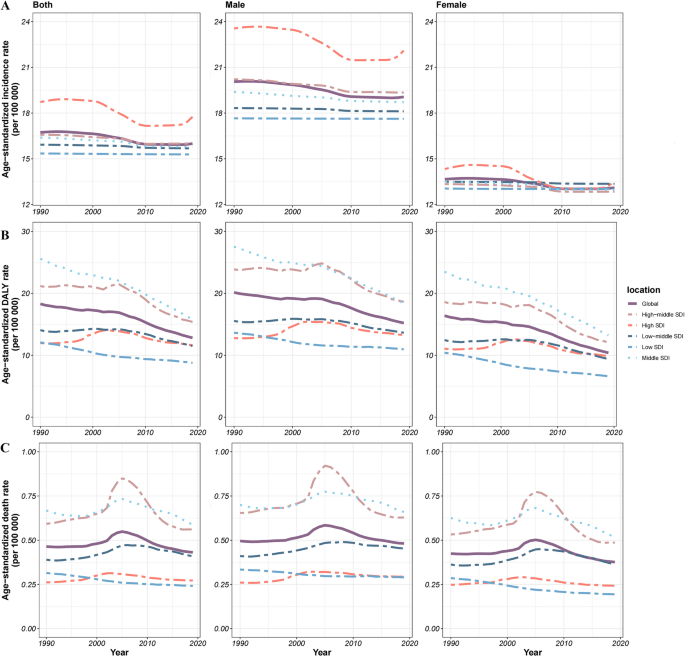
Temporal trends of the age-standardized incidence rate (A), age-standardized DALY rate (B), and age-standardized death rate (C) (per 100,000 persons) for the burden of myocarditis globally and among different SDI quintiles from 1990 to 2019. DALY, disability-adjusted life year; SDI, sociodemographic index
In terms of sex, males and females globally experienced similar trends in ASIR for both sexes from 1990 to 2019. However, males had a greater ASIR than females did in both the global and all SDI regions (Fig. 2A). Notably, the average annual percent change in men decreased faster than that in women in all locations except for the middle of the SDI (Fig. S1A).
DALY and mortality burden of myocarditis from 1990 to 2019
Generally, the age-standardized DALY rate and age-standardized death rate (ASDR) in the global and all SDI quintiles declined (Fig. 2B&C). The middle-SDI quintile had the highest age-standardized DALY rate and ASDR, which were higher than the world average; conversely, the low-SDI quintile had the lowest age-standardized DALY rate and ASDR. Remarkably, between 2002 and 2015, the ASDR presented a transient rise and decline in high-middle SDI regions; even in this zone, the ASDR peaked in 2005 (Fig. 2B&C). Countries with a middle SDI had a faster decrease than those with a high SDI, with average annual percent changes of −1.64 (95% CI= −1.71 to −1.57) and − 0.07 (95% CI= −0.21 to 0.07), respectively. Compared with those in countries with four other SDIs, the ASDRs in countries with low SDIs decreased faster, with an average annual percentage change of −0.91 (95% CI=−0.95 to 0.87).
By sex, males achieved a higher age-standardized DALY rate and ASDR than females did in all regions (Fig. 2B&C). Notably, the decline in the average annual percent change in females was greater than that in males in both the global and four SDI quintiles. Conversely, males experienced a positive average annual percent change at high SDIs (Fig. S1B&C). However, regardless of sex, only the ASDR was positive at a low-middle SDI, whereas the DALY was not. Curiously, the average annual percent change in females decreased faster than that in males globally, with high-middle-SDI, middle-SDI, and low-SDI values, but the average annual percent change in males was significantly positively associated with high-SDI values (Fig. S1B&C).
Incidence, DALY, and mortality burden of myocarditis in adolescents and young adults from 1990 to 2019
With increasing age, the difference in age-specific (15–39 years of age) incidence in both sexes increased globally across all SDI regions from 1990 to 2019. Interestingly, in the same study stage, the age-specific incidence of males resembled that of both sexes in 2019, whereas females had equal incidence rates in the 15–39 age group (Fig. 3 and Fig. S2).
Fig. 3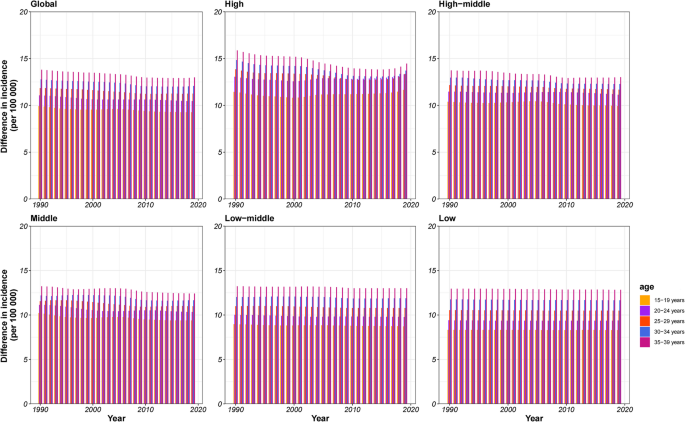
Differences in age-specific incidence in both males and females by sociodemographic index (five categories; countries with high, high-middle, middle, low-middle, or low sociodemographic indices) from 1990 to 2019
From 1990 to 2019, no fixed trends in the global and SDI quintiles were observed, except for low SDI in different age groups. However, countries with high-middle SDIs between 35 and 39 years had the highest DALY rates in both sexes. Interestingly, for both sexes, countries with low SDIs had the highest DALY rates in the 25–29 years age group and the lowest rates in the 30–34 years age group during the same period. While the age-specific incidence differed between males and females, the age-specific DALYs of males resembled those of both sexes in 2019. For females, the DALYs were equal across all five age groups during the study period (Fig. 4 and Fig. S3).
Fig. 4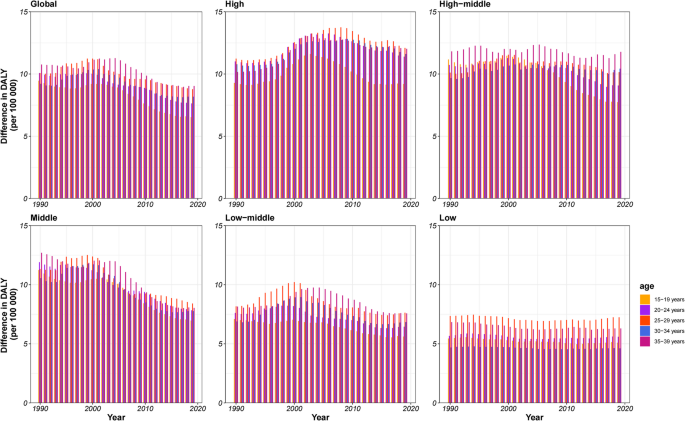
Differences in age-specific DALYs in both males and females by sociodemographic index (five categories; countries with high, high-middle, middle, low-middle, or low sociodemographic indices) from 1990 to 2019. DALY, disability-adjusted life year
In general, at 35–39 years and 15–19 years, the mortalities in both sexes were the highest and the lowest, respectively, globally and in the five SDI quintiles from 1990 to 2019. Notably, the mortality rate from 25 to 29 years in both sexes increased rapidly, approaching the age range of 35–39 years in countries with a low SDI between 1990 and 2019. As with incidence and DALY, the difference in the age-specific mortality of males was similar to that of both sexes in 2019, whereas the mortality of females was equal across the five age groups during the same study stage (Fig. 5 and Fig. S4).
Fig. 5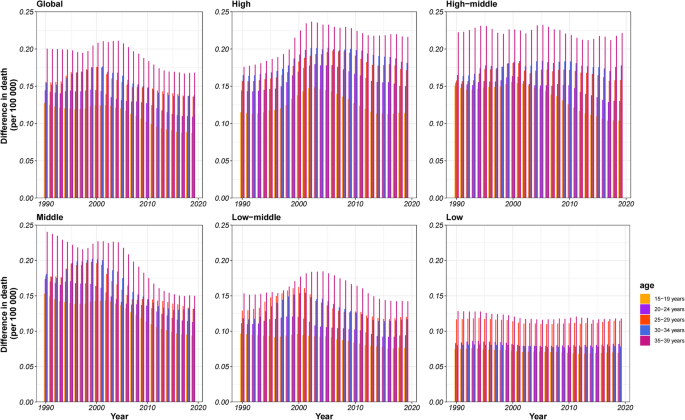
Differences in age-specific deaths in both males and females by sociodemographic index (five categories; countries with high, high-middle, middle, low-middle, or low sociodemographic indices) from 1990 to 2019
Prediction of the prevalence, incidence, DALY, and mortality burden of myocarditis in adolescents and young adults between 2020 and 2030
We categorized the myocarditis data into five age groups (15–39 years) grouped by different SDIs. Globally, the prevalence and incidence of myocarditis in these five age groups will maintain a steady trend between 2020 and 2030, and the incidence will continue to increase with age. However, in the high-middle-SDI group, the highest level of prevalence was in the 20–24 years age group (Fig. 6), and the highest level of incidence was in the 35–39 years age group (Fig. S5). Furthermore, we also grouped myocarditis by sex to assess the number and ASR of prevalence and incidence in different regions. The prevalence and incidence of ASR will still be higher in men than in women in different regions between 2020 and 2030 (Fig. S8 and Fig. S9).
Fig. 6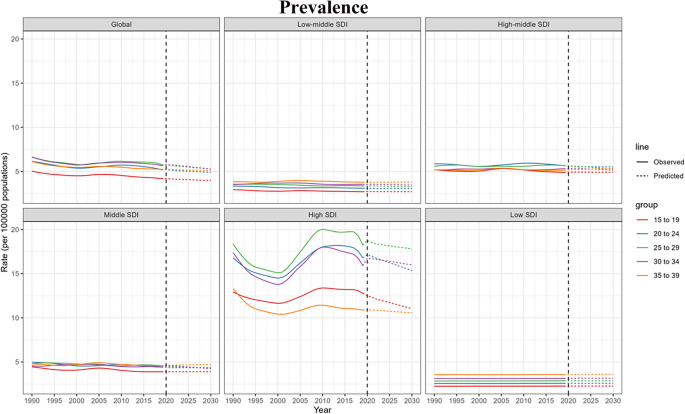
The prediction of age-specific prevalence in both males and females by the SDI (five categories; countries with high, high-middle, middle, low-middle, or low SDIs) from 2020 to 2030. SDI, sociodemographic index
We also divided the myocarditis data into five age groups; at the same time, we marked the data with different locations of myocarditis. Globally, we predict that the DALY of myocarditis will decrease between 2020 and 2030, except that the DALY of 15–24 years will be stable (Fig. S6). Similarly, we predicted that the ASR and number of DALYs would still be higher in men than in women in different regions between 2020 and 2030 (Fig. S10).
Across the globe, we predicted that the mortality of myocarditis would decrease in each age group we studied between 2020 and 2030. Notably, the mortality of myocarditis would remain stable in each age group we studied in countries with a low SDI between 2020 and 2030 (Fig. S7). Similar to the increase in incidence or DALY reported here, the number and ASR of deaths would still be higher in men than in women in different locations between 2020 and 2030 (Fig. S11).