
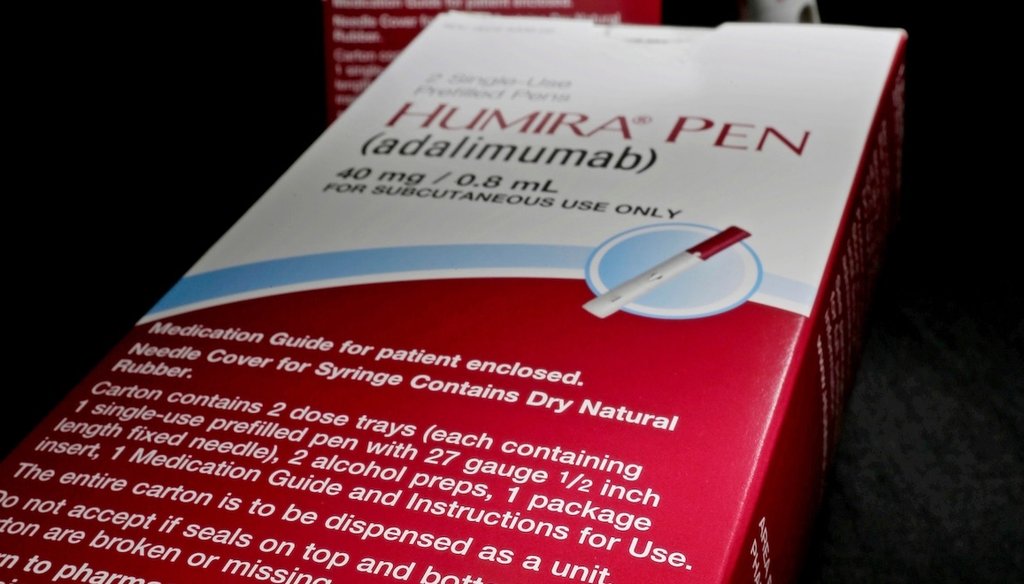
If you watch TV and don’t mute ads, you’ve probably heard of a few biologics. They’re drugs such as Humira for arthritis and Trulicity for Type 2 diabetes.
You may also know they are expensive. Biologics represented 5% of the drugs prescribed in the U.S. in 2024, but they accounted for more than half of the country’s total prescription medicine spending, according to health data analysis company IQVIA.
The Trump administration said it hopes to make these medications more affordable partly by increasing access to “biosimilars,” or highly similar products. What are biologics and biosimilars and will the administration’s proposals help drive down their costs?
Q: What are biologics?
A: Biologics is short for biological medications or products. It’s a broad category of products that include vaccines, blood and blood components, gene therapy and tissues. They are a class of complex drugs produced through biological processes or from living organisms such as proteins and genes. They treat cancer, autoimmune diseases and other rare disorders.
Biologics are typically administered by injection or through an intravenous infusion, said Alex Keeton, executive director of the Association for Accessible Medicines’ Biosimilars Council, an industry group that advocates on behalf of biosimilar manufacturers.
The FDA approval process for these products is rigorous and typically takes 10 to 15 years, said Brian Chen, a University of South Carolina health law and economics expert. Speedier timelines are possible in extraordinary circumstances: Federal agencies worked with vaccine manufacturers and scientists to expedite COVID-19 vaccines, for example.
Q: What are biosimilars?
A: As the name suggests, these medications are similar to the original biologics approved by the FDA. Biosimilars are developed and sold after the original biologic has lost its patent exclusivity, Keeton said. Biosimilars for Humira include Cyltezo, Amjevita and Idacio.
“They still work the same way, clinically, but they’re not exactly the same,” Keeton said.
That’s because, unlike with generic versions of brand name drugs, it’s impossible to make exact copies of biologics. Biologics have complicated production processes and their components are derived from live organisms.
“Biologics are like strands of flexible, cooked spaghetti folded in very specific ways, making exact replication nearly impossible,” Chen said.
The FDA evaluates proposed biosimilar products against the original biologic to determine that the product is extremely similar and has no meaningful clinical differences. It is expected to have the same benefits and risks as the original biologic. To be approved, biosimilar manufacturers show that patients using their products don’t have new or worsening side effects compared with patients using the original biologic.
FDA approval for biosimilars often takes five to six years, Keeton said.
Biosimilars also increase market competition, incentivizing brand name drug manufacturers to lower their prices.
Q: How much do biologics and biosimilars usually cost?
A: They’re pricey, but exact costs vary.
One 2018 study found that biologics and biosimilars can cost a U.S. patient $10,000 to $30,000 each year on average.
Humira was listed at $6,922 in early November. The Humira biosimilar Cyltezo advertises for 5% off Humira’s cost; the makers of Cyltezo also offer a non-brand name option for people who pay cash at pharmacies while using GoodRx at a price of $550.
The actual amount an insured patient pays also depends on their plan and their insurer’s negotiated rates.
Biosimilar prices typically run 15% to 35% lower than their brand name biologic counterparts, one 2024 study reported. The FDA found biologics produce a more dramatic cost savings of 50% on average.
Q: Why are these medications so expensive?
A: Biologics and biosimilars are difficult to develop and produce, which adds to their expense.
Making a standard over-the-counter medication such as aspirin requires five ingredients. Making insulin, a biologic, requires genetic modifications to living organisms.
These complex manufacturing procedures and proprietary information make it difficult for competitors to create alternatives.
To put this in perspective, there were 226 marketed biologics in the U.S. as of July 2025, and the FDA had approved 76 biosimilars such as insulin. When it comes to non-biologic medications, the FDA has approved more than 32,000 generic drugs — that’s more than the number of approved brand name drugs.
Q: Can biosimilars be used in place of the original, FDA-approved biologics?
A: Yes. All biosimilars must meet FDA requirements and show that their products are highly similar and have no clinically meaningful differences from its existing FDA-approved biologic counterpart.

The Food and Drug Administration campus in Silver Spring, Md. on Oct. 14, 2015. (AP)
Q: So how does the Trump administration hope to change the FDA approval process for biosimilars?
A: Under its draft guidance, the administration proposed reducing some of the tests required as part of the FDA process used to prove a biosimilar drug is as safe and effective as its biologic counterpart.
Previously, a manufacturer requesting a biosimilar license had to provide clinical study data proving its product’s similarity. The FDA’s new proposal would no longer require drug developers to conduct these comparative clinical trials.
Manufacturers would still be required to test proposed biosimilars. Other data — including comparative analysis, immune response data and human study data showing how the drug moves through the body — could sufficiently demonstrate the drug’s similarity to an existing biologic, the FDA said.
Q: Why does the FDA want to change the biosimilar approval process?
A: Ultimately, the agency said it aimed to incentivize drug manufacturers to quickly develop biosimilars by eliminating redundant, costly and time-consuming clinical studies, Keeton said.
Saving that time might increase the number of biosimilar alternatives.
It will almost certainly lower the front-end development costs for drug makers, Chen said.
Q: Will that change lower the costs of these medications for patients who need them?
A: Regulatory changes alone may not significantly drive down prices for the average American.
Several non-brand name options need to be available in order to produce significant price drops, according to a Department of Health and Human Services report.
But prices could remain the same even with more options.
A 2024 JAMA Health Forum study found that annual out-of-pocket costs either increased or remained stable for most biologics even after biosimilars were available. Patients who used biosimilars didn’t pay less than those who used the original biologics.
That’s at least partly because biologic manufacturers often offer substantial rebates to pharmacy benefit managers, companies that work with insurers, employers and others to manage prescription drug plan benefits. In exchange, insurers give the name brand biologics preferred or exclusive placement on their lists of insurance-covered drugs, Chen said. Rebate walls ultimately prevent the sale of cheaper biosimilars, he said.
Q: Are there any other obstacles to getting more biosimilars on the market?
A: Yes, another key hurdle remains: Name brand biologic manufacturers often hold many patents and file lawsuits blocking approved biosimilars from being commercially marketed.
Chen’s 2018 study found that of 12 FDA-approved biosimilar products as of October 2018, five were commercially available. Six others were unavailable because of patent disputes.
PolitiFact Researcher Caryn Baird contributed to this report.
RELATED: Fact-checking Democrats’ talking points about Affordable Care Act subsidies
RELATED: Donald Trump exaggerates speed, certainty of prescription drug price reductions