


“Brain health isn’t something that we only worry about in old age. We need to be thinking about brain health all through our lives.” — Dr Etuini Ma‘u, old age psychiatrist, dementia researcher, and senior lecturer in psychological medicine at Auckland University. (Photo: Mark Hamilton)
With the number of over-65-year-olds in Aotearoa set to hit the million mark by 2029, many of us will already know someone with dementia. It’s a sure bet, too, that we’ll be coming across the work of Dr Etuini Ma‘u, an old age psychiatrist, dementia researcher, and senior lecturer in psychological medicine at the University of Auckland.
Here he is talking to Dale Husband, about why we should be thinking about our brain health now.
Tēnā koe, Etuini. Thank you for agreeing to share some kōrero with us about your life and work. I’m really interested in your research work on dementia and the cognitive decline that happens as we get older. But first, tell us a bit about your clan, please, Etuini, and the names you carry.
My full name is Etuini Scipio ‘Alofaki Ma‘u. My father, Paula, is Tongan. He’s from Kolomotu‘a in Tongatapu and Masilamea in Vava‘u. And my mother is Jennifer, and she’s Pālangi. She came to Tonga in the early 1970s to teach. Met Dad there, and the rest is history.
I’m named after both my grandfathers. Etuini is Tongan for Edwin, after my maternal grandfather, Howard Edwin Harkness. Koliniusi Sikipio Ma‘u is the name of my paternal grandfather, after the Roman general Cornelius Scipio Africanus. Dad decided he wanted the Latin spelling for my name, so that’s why I’m Scipio. ‘Alofaki-he-lotu is the name of our home in Kolomotu‘a.
My mum’s family has a long relationship with Tonga. Her granddad was there as a missionary back in the early 1900s, so my grandfather, Edwin, was actually born in Ha‘apai.
I love the way our Pasifika people honour previous generations by bestowing names on our tamariki. I have some connections there because our mokopuna are from Kolovai, and so I have a great affection for Tongan communities and Tongan people. But isn’t it wonderful that previous generations are celebrated in the ingoa that our people carry forward?
Yes, absolutely. I have no recollection of either of my grandfathers, but it’s humbling to be named after two men who were very strong in the church. Both of them were ministers. Edwin was in the Methodist Church of New Zealand and Sikipio in the Free Wesleyan Church of Tonga.
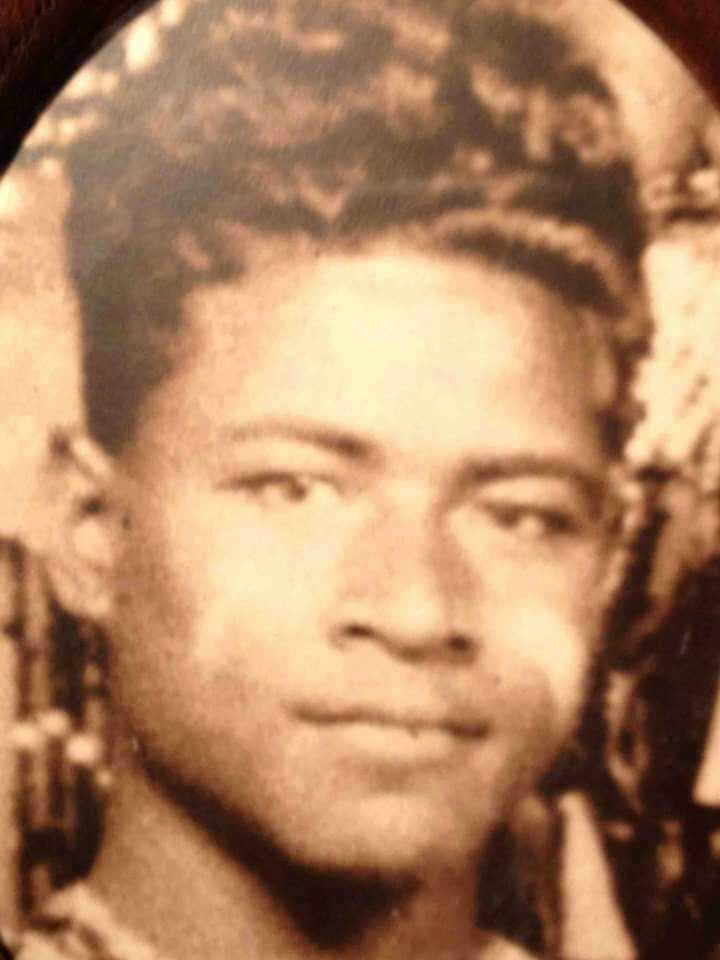
Etuini’s paternal grandfather, Rev Sikipio Ma’u, was named after the Roman general Cornelius Scipio Africanus. (Photo supplied)
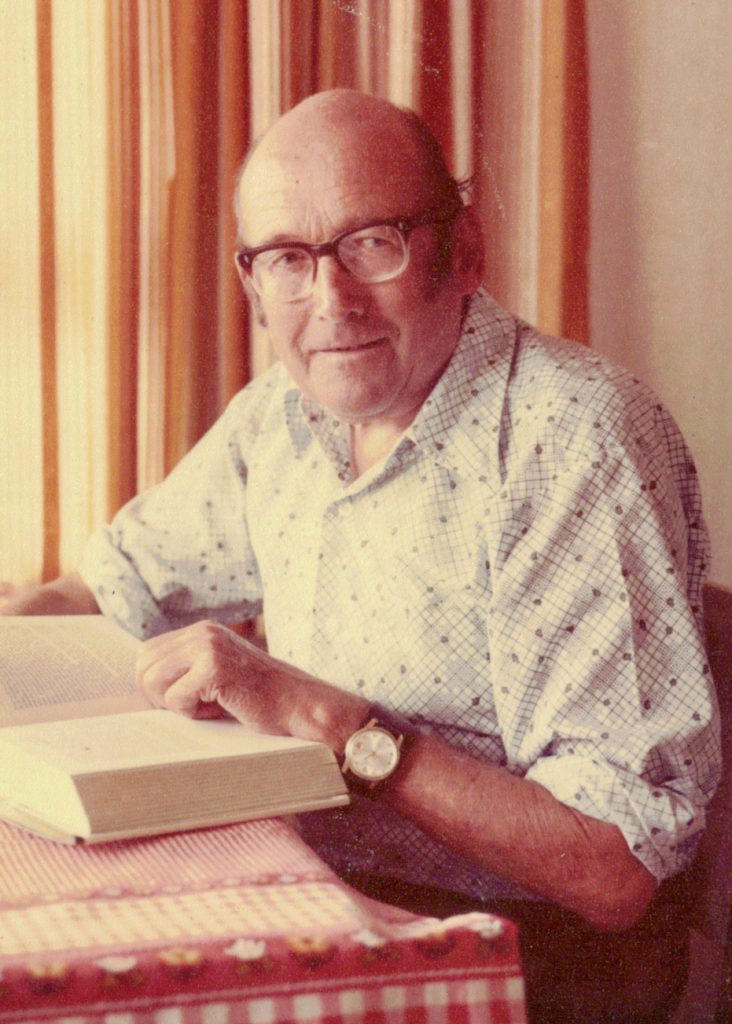
Etuini’s grandfather on his mother’s side, Rev Edwin Hardness, was born in Ha’apai, Tonga. His father went to Tonga as a missionary in the early 1900s. (Photo supplied)
But you were born here in New Zealand — and your dad and mum were teachers?
Mum’s actually a nurse, but she went to Tonga as a missionary for the Methodist Church and taught at Queen Salote College. My father was born and raised in Tonga and taught at Tupou College for many years.
I was born in Tonga, and I did most of my schooling there until the end of the fifth form. I went to Tonga Side School and Tonga High School, and left after I got School Certificate. I did my sixth and seventh form years at Wesley College, out in South Auckland, before going to med school at Auckland University.
So you’re a fluent speaker of the Tongan language. Is this a taonga for you in life, that you’re able to converse comfortably in te reo Tonga?
Absolutely. It’s interesting, though. Tongan is a compulsory subject at Tonga High School, but I had friends who were either Pālangi or Pālangi-Tongan who got exemptions so they wouldn’t have to do the Tongan class. So I am forever grateful to my parents, even though I hated it at the time, for saying: “No, you go and learn Tongan, and you participate in everything.”
Looking back, that was probably the best decision they made because I can speak the reo. I’m not a confident orator, because I left at 15, but it’s certainly useful to be able to speak and read Tongan.
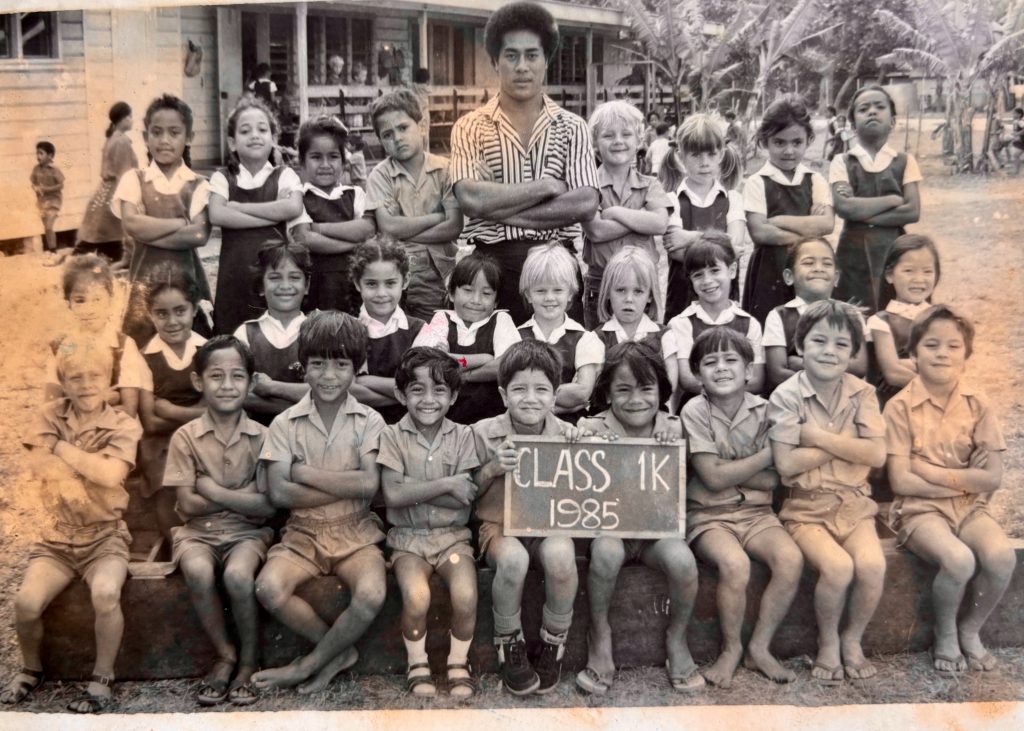
Tonga Side School Class 1, in 1985. Etuini is in the front row, third from right. (Photo supplied)
![]()
“One of my proudest moments was getting detention for speaking Tongan at school.” Pictured: Etuini (second from right) in Form 1 at Tongan High School, 1991, with his sister Sikimeti (far left), his brother Sione, and a school friend. (Photo supplied)
You know, I’ve often noted that people who diss new arrivals from the islands for their “fresh” accents overlook the fact that they’re bilingual, while most of the ones making fun of them are monolingual. Did your time at Wesley help you to get comfortable with the English language?
In fairness, English was my first language. Mum made a big point of us speaking English at home because we were surrounded by the Tongan language.
But at Tonga High School, we weren’t allowed to speak Tongan on the school grounds — it was English only, and it was strictly enforced. One of my proudest memories was getting detention for speaking Tongan at school.
Wesley was a melting pot of Pasifika guys, and I know it’s been going through the mill a little bit recently, but that can happen with boarding schools. Māori boarding schools, too. What did you find about the multicultural nature of Wesley when you attended?
I really enjoyed my time at Wesley. When I was there in the mid-90s, there were a lot of scholarship students from around the Pacific. We had people from Tonga, Sāmoa, Kiribati, Papua New Guinea, Solomon Islands, Vanuatu, Tuvalu. And I remain in contact with them 30 years later.
Etuini, was there always an expectation that you’d be going to varsity, or did you sort of set that pathway yourself?
I have an older brother and sister, Sione and Sikimeti, and I think there was always an expectation that we’d study in Tonga until School Certificate, we’d finish high school in New Zealand, and then we’d go to university.
I just kind of followed my brother and sister, and we all did exactly the same thing. We all finished up at Wesley, and then we all progressed on to Auckland uni.
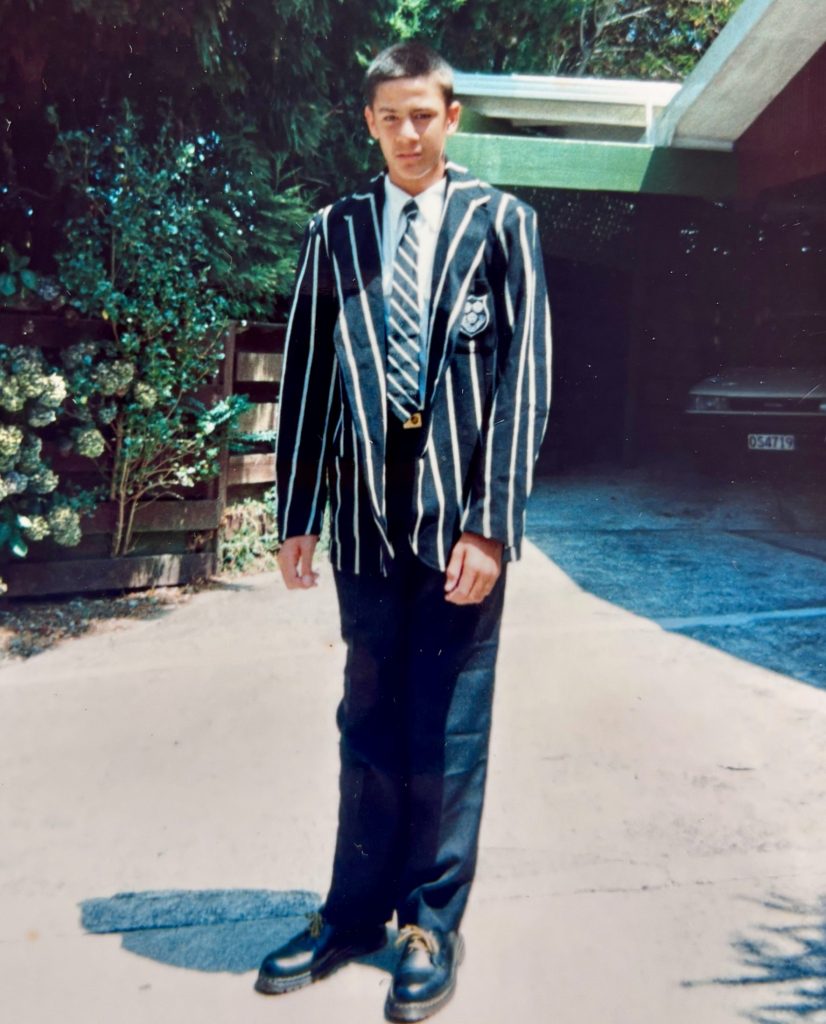
Starting Form 6 at Wesley College in South Auckland in 1996. Like his older brother and sister, Etuini did his senior years at Wesley. (Photo supplied)
Pretty high-achieving family by the sound of things, mate. Did you follow in your siblings’ footsteps?
Dad was a maths teacher, so both my brother and sister have done their doctorates in maths. I went down a different line and did medicine instead. But now, with some of the research I do and a lot of the data analysis, I think the maths background does come in handy.
Did you always hope during your studies that one day you’d be able to contribute to improving Pasifika health?
I went into medicine straight out of high school. And, hand on heart, when you’re 17 going on 18, starting your first year of a medical degree, you have very little worldview, and very little understanding of how the health system works, or of health in general.
So, in a way, you go into it fairly blind, with a very idealistic view of what medicine is. I mean, it was a six-year medical degree. You kind of just ground your way through six years of study to come out the other end.
There’s been quite a focus on Māori health and on programmes designed to support a more Māori approach to achieving better health statistics for our people — and I guess many Pasifika students have been drawn into that more recent approach. Is that the case with you in your work? Has it been beneficial to look across at these developments in Māori health as you consider alternatives to improving Pasifika health?
I’m very fortunate, Dale. I married one of my classmates, Jade Tamatea. She’s a Māori endocrinologist and academic, and I think a lot of my views on health equity, health outcomes, and Pacific and Māori health have been shaped by her passion and drive for improving Māori health.
I’ve taken a lot of what I’ve learned from her and from the environment that she works in, and started applying it to Pacific people and my research.
Well, that’s a rare thing, isn’t it, Etuini? Finding love in the lecture theatre. When you graduated with your ticket to be a doctor, so to speak, were you looking at being a GP, or did you already have a specialty in mind?
At med school, I’d been thinking about doing something like paediatrics, but in my final year as a student, I had a really good experience in psychiatry.
I had a great supervisor, Dr Shailesh Kumar, and his passion and enthusiasm for teaching made me think I’d give psychiatry a go. So, I went back and did my first-year of psychiatry training in Rotorua with him, and then Jade and I moved up to Waikato to finish our specialist psychiatry and physician training.

On a sabbatical in Tonga, in 2019, with Dr Mapa Puloka (white coat), Dr Pita Pepa (in blue) and a visiting Chinese psychiatrist. Dr Puloka was Tonga’s only psychiatrist for three decades. (Photo supplied)
I’m always nervous when we talk with psychiatrists . . .
Yeah, I hear that a lot!
It’s a fascinating area, though. I’m very interested in the areas that you’ve studied — not only in the human mind and its amazing powers and abilities, but also dementia and the cognitive decline that we’re witnessing as we live longer. What led you to that area of study, Etuini?
After I went into psychiatry, I decided to specialise in the psychiatry of older people. So, predominantly focusing on people over 65. We know that things like dementia and cognitive decline become more common as you get older. So, about a third of my work is dealing with people with dementia and difficulties with their cognition.
It’s nearly 10 years now, Dale, since the report of the first Lancet Commission on Dementia Prevention came out in 2017. At the time, there was a lot of fanfare around it because there was finally enough evidence to say, “Here are nine risk factors that we could potentially address that would reduce the rates of dementia in the longer term.”
I remember thinking: “Wow, actually, dementia isn’t an inevitable decline as you get older. There are things that we can do.” I think that’s when my interest and passion started shifting toward dementia prevention.
I’m interested in your focus on bilingualism as a tool to stymie cognitive decline. But there are also issues of loneliness that are a very real part of modern life for many. And I suspect that the decline in social interactions can also contribute to cognitive decline. Are we seeing rising rates of dementia, or mate wareware, and what do you put this down to, Etuini?
The easy answer is that we’re living longer and our population is generally ageing. So, most of the increase in the number of people with dementia, in Aotearoa, in the world in general, is because we’re getting older as a society, and we know that dementia is fundamentally a disease of older people.
I think the issue, Dale, is that we need to move from thinking about dementia being a disease of older people to thinking about dementia and the symptoms of dementia as being the end result of cumulative and incremental damage sustained to the brain over a lifetime that eventually overwhelms our brain’s ability to cope.
We know, for example, that our brain is only about a kilo of our body mass, but it uses about 20 percent of our body’s nutritional needs. So, anything that affects our heart, that affects blood flow to the brain, is going to affect the brain. And that’s why all of those physical health risk factors are there — diabetes, obesity, hypertension, smoking, alcohol, and so on.
But you’ve also touched on a really important aspect — and that’s our cognitive reserve, our cognitive resilience, our brain’s ability to compensate and to keep functioning normally, even when we have those changes happening. And that’s all about how we keep our brains active and stimulated.
So, things like bilingualism are really important because we know that the more you use your brain to think in different languages, the more you strengthen it. We know that interactions with other people strengthen it, too, so social isolation and loneliness become risk factors.
And we know that anything that affects our ability to interact and connect with other people — things like hearing and vision loss and depression — is going to increase our isolation as well.
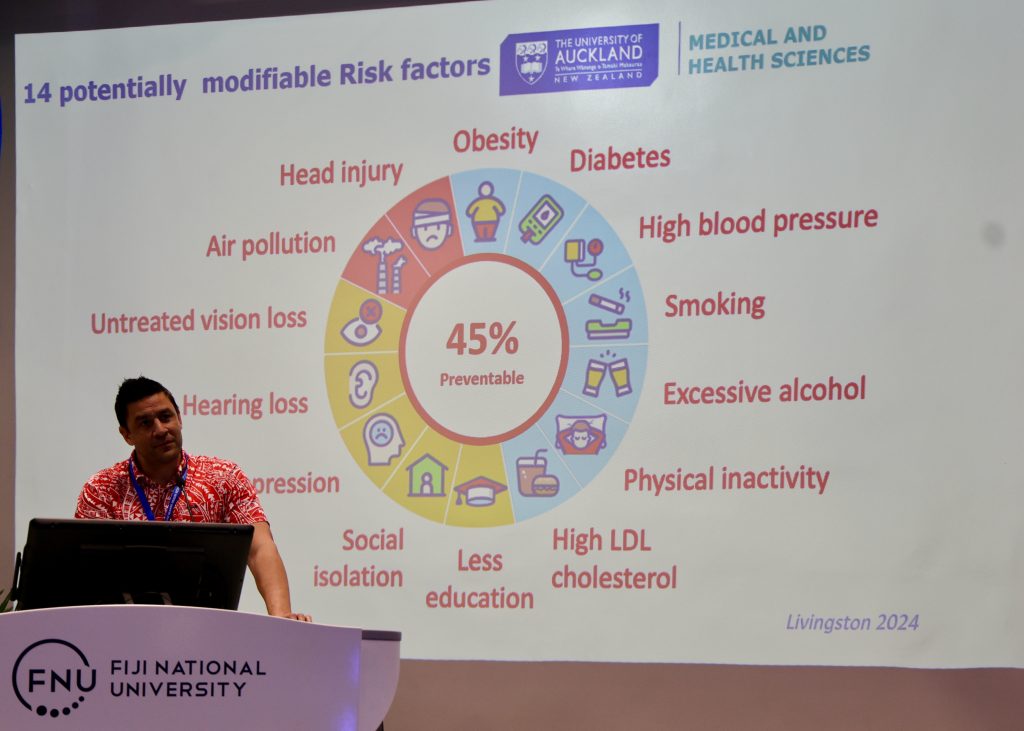
Etuini presenting dementia prevention research findings in Suva, Fiji, 2025. “If we can catch people early in the dementia process, there are things that can be put in place. Things like cognitive stimulation therapy and anti-dementia medications that won’t stop or reverse the progression of dementia, but can slow the rate of decline.” (Photo supplied)
Many whānau, including our own, have little understanding of the brain function. When you think of whānau for whom dementia or cognitive decline is a reality, how important is it that they understand what’s happening so they can modify the way that they awhi and support that person in ways that they hadn’t considered before?
The first thing I’d say, Dale, is that what’s really important is that we improve awareness in the community. Cognitive symptoms and changes in memory aren’t a normal part of ageing — but they’re potentially part of a process that could progress with time.
The reason I bring that up is because we know that if we can intervene early, if we can catch people early in the dementia process, there are things that can be put in place. Things like cognitive stimulation therapy and anti-dementia medications that won’t stop or reverse the progression of dementia, but can slow the rate of decline.
Caring for someone with dementia is hard. And one of the hardest things for families to grapple with is how to manage someone whose understanding of the world around them, and how they interpret what’s happening, is just so different from what it used to be.
The onus is on carers, families, and health professionals to make changes to that person’s environment and to change the way that we interact with them. Because we know they aren’t able to change anymore.
Have you seen any significant differences, Etuini, between the Tongan community growing up here New Zealand with the predominantly western lifestyle, and the Tongan community back at home? Are there differences in the stats between people growing up in two vastly different communities and societies?
It’s a good question, Dale, but I don’t have the answer. One of the difficulties with researching Pacific populations is that we have two or three very distinct groups. We’ve got the group who came for employment as part of that great migration of Pacific people in the 1950s and 1960s. And we also have second- and third-generation Pacific communities who’ve been born and raised in New Zealand.
So, it’s really hard to draw those parallels. Anecdotally, if we look at, for example, Tonga, there are differences in the social fabric, in the ability to engage with your community, with your church, and to get that kind of social stimulation.
Some of my colleagues talk about families they’ve seen who, with the best intentions, bring mum and dad to New Zealand because they want to look after them. But then they go to work, and mum and dad are more isolated than they were at home. Usually, they can’t drive, and you can’t just walk down the road to engage with your local church or community.
So, while the intentions are really well placed, sometimes they’re removing people from a community where they were getting that social connection and stimulation.

The mental health team of PACMAT (Pasifika Medical Assistance Team) deployed to Tonga by the Pasifika Medical Association) after the Hunga-Tonga/Hunga Ha’apai eruption and tsunami in 2022. From the front: Fane Uasi, Sela Vailala, Makoni Havea, Etuini, Tuilavoni Lama, Netane Takau. (Photo supplied)
One thing I was intrigued by, too, was that you’re delving into the economic impact of dementia for your PhD research. What were some of your findings there, on the economic impact of dementia, and the inaction to address these types of issues?
Look, the economic impact of dementia is massive, and it disproportionately affects our Pacific community and our Māori community. The reason for that is that most of the cost of dementia care in New Zealand is based around people going into aged care, into rest homes.
And we know that those rest homes are designed for the Pālangi majority. We know that those rest homes aren’t seen as fit for purpose, or appropriate, or acceptable, by our Pacific and Māori communities. So Pacific and Māori families are three times less likely to be using that aged care.
The problem is that not using that care isn’t compensated for by receiving more care to look after someone at home. So that’s where the inequity and cost comes in. And if the cost isn’t being covered by the Ministry of Health, by the state, then it’s falling on the families themselves. That inequity is something that we really need to focus on.
There’s been a strong push, as you’d be aware, to have experienced Māori researchers working on research about Māori. With that in mind, I’m just wondering what you think about the importance of culturally focused research. Why is it important, and what’s some of the most significant work you’ve been exposed to that brings a cultural perspective into its findings?
A lot of the work I’ve done over the last six years has been around quantifying the level of risk in our Pacific communities for dementia, modelling what that looks like over time, and trying to understand the key drivers.
From a dementia prevention point of view, Dale, what we’ve shown very clearly is that there is nothing innately risky about being Māori or Pacific that increases your risk of dementia. The main driver is the fact that our communities are generally poorer and live in areas of higher socioeconomic deprivation.
We’ve shown that Pacific people who live in the most affluent areas in New Zealand have the same low risk as Pālangi who live in those affluent areas. We’ve shown that Pālangi who live in the poorest areas of New Zealand have the same high risk as Pacific and Māori communities who live in areas of high social disadvantage and deprivation.
That tells us that there is nothing inherently Pacific or Māori that is increasing our risk. It’s all being driven by the fact that we’re overrepresented in areas that are poorer and more disadvantaged. So, the solution for that isn’t at the level of the individual. The solution for that is actually thinking about how we can change their environments to improve their situation.
We know that vape stores, fast food outlets, and alcohol outlets all cluster around areas of higher deprivation. We know that access to parks and green spaces, to cycle lanes, to adequate public transport tends to be less available in poorer areas.
I think the only way we’re going to meaningfully effect change is by changing those environments. Then we can help people make unconscious choices that are healthy, rather than expecting them to change despite their environment telling them something else.

At daughter Te Paea’s Certificate in Health Science graduation in 2025. From left, mother-in-law Karen Tamatea, Te Paea, wife Jade Tamatea, and Etuini. (Photo supplied)

Etuini’s son, Lisiate, and father, Paula, at Paula’s 90th birthday, November 2025.
And to effect that change, we need advocacy. What would you say about the interest that’s been shown in young people like yourself, Etuini, by those who are conscious that there are moves we can make to address cognitive decline and dementia, but it takes sustained approaches, adequate resourcing, and ultimately strong advocacy. Are you enthused by the calibre of people who are interested in this field?
Absolutely. There’s growing recognition that we need to be addressing things at a population level, at a societal level. I’m certainly very grateful to people like Catherine Hall at Alzheimers New Zealand for taking a lot of our research findings and getting them in front of politicians.
We actually had a meeting with some Friends of Dementia parliamentarians about a year ago, Dale. It was really interesting because I was telling them about the impact of poverty and social disadvantage on dementia risk, but that kind of ended up in the too-hard basket. They were more interested in some of these newfangled medications, that, one, are very expensive, and two, don’t have much benefit.
So that was a bit disheartening because it showed that politicians are more interested in immediate solutions.
There is no immediate solution for dementia prevention. We need to take a long view — 10, 20, 30 years into the future. We need to be thinking about interventions and initiatives that don’t fall within a three-year political cycle.
It’s very humbling when you witness the slow cognitive decline of somebody that you love. Sometimes it’s rapid. But we can learn from them still. Even though it might seem that we’re caring for them, in some ways, the lessons of humility, the lessons of aroha that they provide, shouldn’t be left out of our thinking.
Caring for someone with dementia takes an emotional toll on families because you’re watching someone you love slowly change from the person that you knew.
I lived with my father-in-law, Peter, for many years, and his dementia evolved over time. I could talk the talk at work and dish out all the advice to my patients and their families, but it was a very different story when I walked in the door at home.
Yeah, it’s a reality check, but it’s something that we take on because of the love and care we have for each other. Is there something else that you’d like to share with those who’ll be reading this ?
For me, the key message is that brain health isn’t something that we only worry about in old age. We need to be thinking about brain health all through our lives. This isn’t about changing our lifestyle in our 50s and 60s as we’re approaching retirement. It’s about recognising that the changes that happen, happen gradually and slowly over many, many decades.
And if we can make the changes earlier in life, in our lifestyles and in our family environment, that’s what will stand our future in good stead.

Jennifer and Paula Ma’u, Etuini’s parents, with all three children and six grandchildren, in 2022. (Photo supplied)
Tēnā koe, Etuni. In interviews like this, we talk a lot about the work we do, but not necessarily the things that we love doing. And I wonder if there’s something that you do that keeps you enthused about life, about work, about family life? What are the things that keep you fresh?
I’m a very slow runner, but I enjoy running because it clears my mind. I enjoy hanging out with my kids, although they’re now a lot older and don’t really want to hang out with Dad much anymore. That’s it, really.
It’s been lovely talking with you, Etuini. All the best to you, and thank you for the important work you’re doing.
Mālō ‘aupito, Dale.
(This interview has been edited for length and clarity.)
Thank you for reading E-Tangata. If you like our focus on Māori and Pasifika stories, interviews, and commentary, we need your help. Our content takes skill, long hours and hard work. But we’re a small team and not-for-profit, so we need the support of our readers to keep going.
If you support our kaupapa and want to see us continue, please consider making a one-off donation or contributing $5 or $10 a month.