
By Anna Howe, Emma Best and Rachel Webb of 
![]()

To stem further spread, we must build on the lessons from New Zealand’s last major measles outbreak in 2019.
Photo: Fiji govt/Facebook
The recent confirmation of new measles cases unconnected to international travel suggests the highly contagious disease has likely started spreading through communities, according to Health New Zealand.
This is a stark reminder of the pending danger of a larger measles outbreak. To prevent transmission once the measles virus has been introduced, a population immunity of around 95 percent, evenly distributed throughout communities, is necessary.
New Zealand does not have this level of vaccination coverage and the main way to prevent an outbreak now is to focus on increasing the immunity of children and on closing the “immunity gap” in the population.
While New Zealand has used the measles vaccine since 1969, a national immunisation register was only introduced in 2005. Without a national register to provide the historical immunisation record, estimates are that only around 80 percent of people born in the 1980s and 1990s are protected against measles.
Although vaccination rates of children have at times reached more than 90 percent since the introduction of the register, the total has never reached the required 95 percent. Immunisation coverage has consistently remained lower among Māori children and more recently also Pacific children.
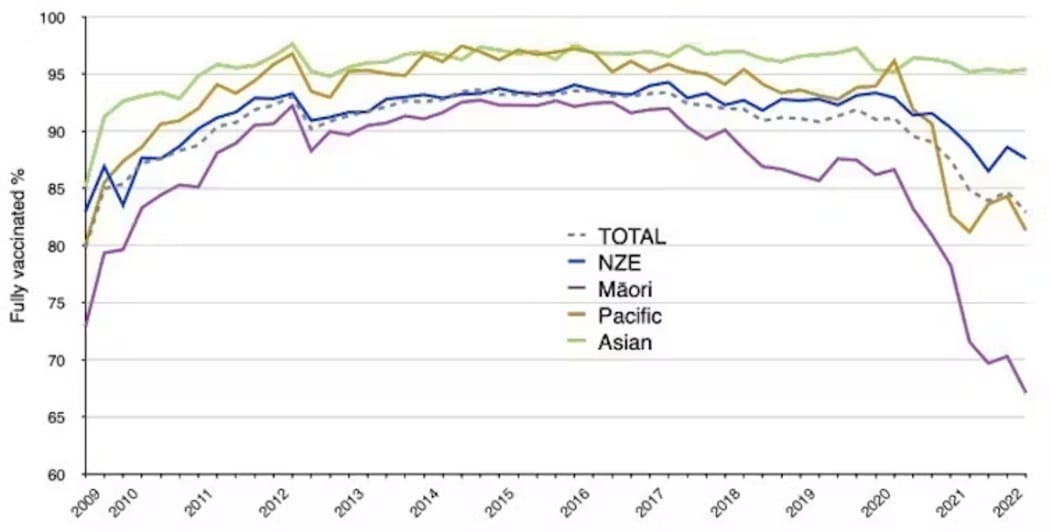
This graph shows that annual immunisation rates for two-year-olds have dropped for Māori and, more recently, for Pacific children, compared to Asian and NZ European (NZE) children.
Photo: CC BY-SA
To stem further spread, we must build on the lessons from New Zealand’s last major measles outbreak in 2019.
That year, Auckland experienced a large and serious measles outbreak – the largest since 1997 – affecting babies, young children and adults. There were more than 2000 cases and about 35 percent required hospital care, despite the fact most people who contracted measles were previously fit and healthy.
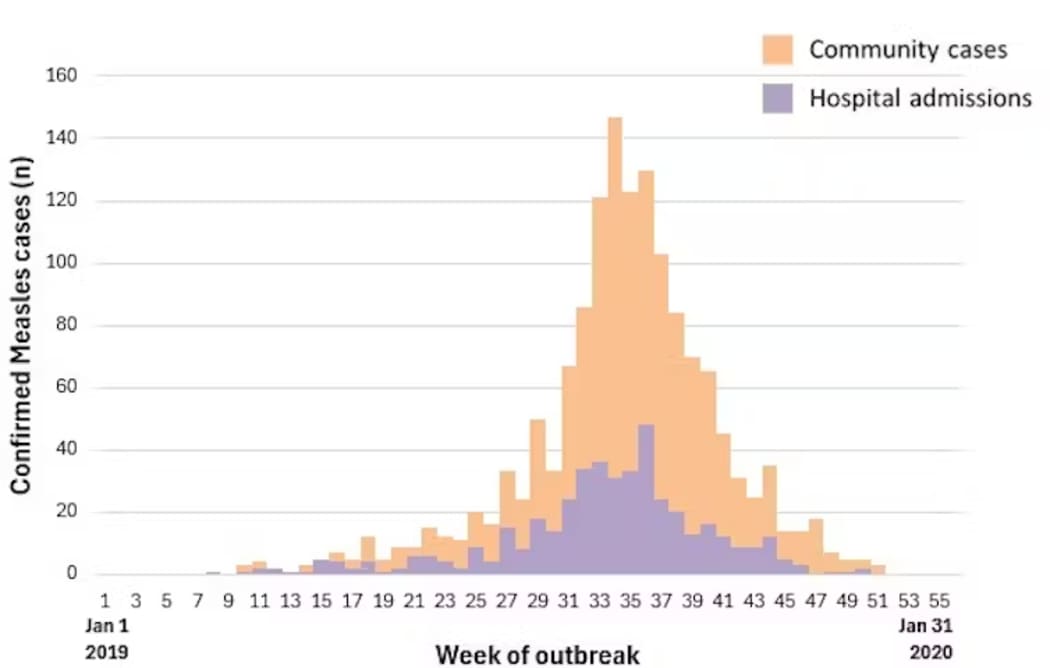
About a third of people under 30 who contracted measles required hospital care during the 2019 outbreak in Auckland.
Photo: CC BY-SA
Some of the serious and lasting complications included encephalitis (brain inflammation), pregnant women losing babies, and children needing lengthy life-saving intensive care.
While acute measles can be severe, our subsequent research shows that measles infection is associated with a long-term increased risk of other infections.
We found that people who had measles in the 2019 outbreak had more hospital admissions not related to measles and more antibiotic prescriptions in the four years following the outbreak, compared to healthy controls.
While the effect was more pronounced for people whose measles infection was severe and needed hospital care, we also saw a lasting effect for those with milder infections.
The severity of this outbreak could have been prevented if more people had been protected with the measles, mumps and rubella (MMR) vaccine.
Immunisation coverage is lacking
Immunisation coverage for the MMR vaccine (given at 12 and 15 months of age) shows New Zealand’s vaccination rates are not enough to prevent an outbreak in children under five.
Data from June 2025 shows only 82 percent of two-year-olds are fully immunised with two doses of the vaccine. This leaves at least one in five unprotected.
Babies under one year of age are not protected because the first MMR dose is only given at 12 months. This is particularly worrying as young babies have very high rates of hospitalisation and complications from measles. In the 2019 outbreak, there were more than 250 cases in babies and more than half of them were hospitalised.
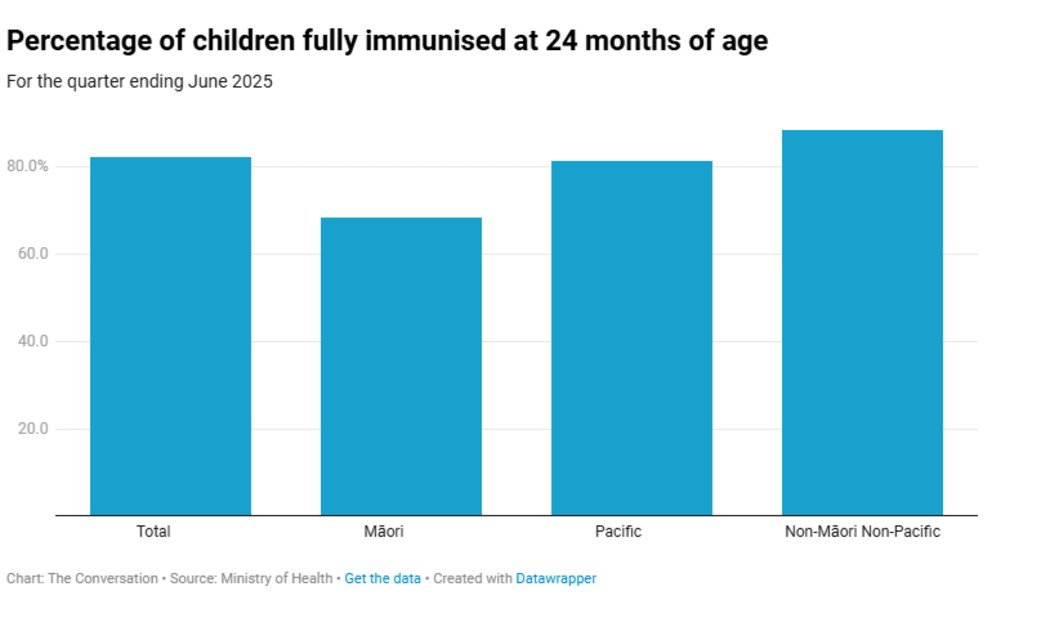
Photo: Ministry of Health
Data also show the burden of the 2019 outbreak was not equitable and these inequities persist in immunisation coverage today. Gaps in coverage create pools of susceptible individuals, rife for measles to take hold and spread.
What is also clear from the recent measles cases is that our history of inadequate measles vaccination has left young adults vulnerable to infection.
This happens at an age when they are able to travel overseas, with the unintentional consequences of bringing measles home to their whānau (family), including unimmunised pēpi (babies).
This would be particularly concerning if a measles outbreak were to take hold before the summer holidays. Even a few cases in New Zealand could make us the source of outbreaks for other Pacific nations.
In late 2019, measles imported from New Zealand resulted in 5700 cases in Samoa, including 1800 hospitalisations and 83 deaths from measles (87 percent of these deaths were children under five).
Awareness and prevention
Anyone under 50 years of age who is experiencing a fever, rash, cough and runny nose should think measles, particularly if they returned from travel in the past three weeks, are unimmunised or a contact of a recent case. They should call HealthLine (0800 611 116) for advice before visiting a GP or hospital, unless severely unwell.
If in doubt vaccinate. The health-sector response to the 2019 outbreak recommended GPs continue to actively recall unvaccinated children after checking the national immunisation register.
For anyone unsure if they have had two doses of the measles vaccine, it is safe to get a dose according to the Immunisation Advisory Centre if they are not immune-compromised or pregnant. MMR vaccines are free and available from GPs, pharmacies and community health providers. Vaccinators are listed on Book My Vaccine.
Measles infection is scary but vaccination can be scary for people, too. The World Health Organization recommends listening with empathy and acknowledging how people who are hesitant are feeling.
It also suggests asking open-ended questions to help understand concerns and sharing evidence-based information from trusted sources, including Health New Zealand or the Immunisation Advisory Centre. It can help to share your own motivations for getting vaccinated and what helped you to overcome concerns.
With a stretched health system and long-term consequences for individuals following measles infection, prevention is essential.
Anna Howe is a Senior Lecturer in Epidemiology at the University of Canterbury.
Emma Best is an Associate Professor in Paediatrics at the University of Auckland, Waipapa Taumata Rau.
Rachel Webb is a Senior Lecturer in Paediatrics in University of Auckland, Waipapa Taumata Rau.
This story was originally published on The Conversation.