
The usual therapeutic dose of fosphenytoin, a prodrug of phenytoin, was administered to a patient with lamotrigine overdose who experienced seizures that did not respond to treatment with sodium bicarbonate and activated carbon. The administration of fosphenytoin shortened the half-life of lamotrigine. Although concomitant phenytoin has been reported to shorten the half-life of lamotrigine at normal therapeutic doses [6], this report is the first to describe the utilization of a phenytoin prodrug as a treatment strategy for lamotrigine overdose. In this patient, phenytoin had not been used concomitantly prior to overdose, but the typical therapeutic dose of fosphenytoin shortened the half-life of lamotrigine in the blood in the setting of lamotrigine overdose. Therefore, fosphenytoin may be an effective treatment for lamotrigine overdose.
The bioavailability of oral lamotrigine is approximately 98%, reaching its highest concentration within approximately 3 hours after oral administration [6]. The half-life of lamotrigine as a single oral dose is 24.1–35 hours [8]. As lamotrigine is metabolized by glucuronidation [9], its blood levels can be influenced by the concomitant use of medications that modulate this process. When combined with carbamazepine, phenobarbital, or phenytoin, which promote glucuronidation, the half-life is shortened to an average of 13.5–15 hours [6]. However, when combined with valproic acid, which inhibits glucuronidation, the half-life increase to an average of 48.3 hours [6].
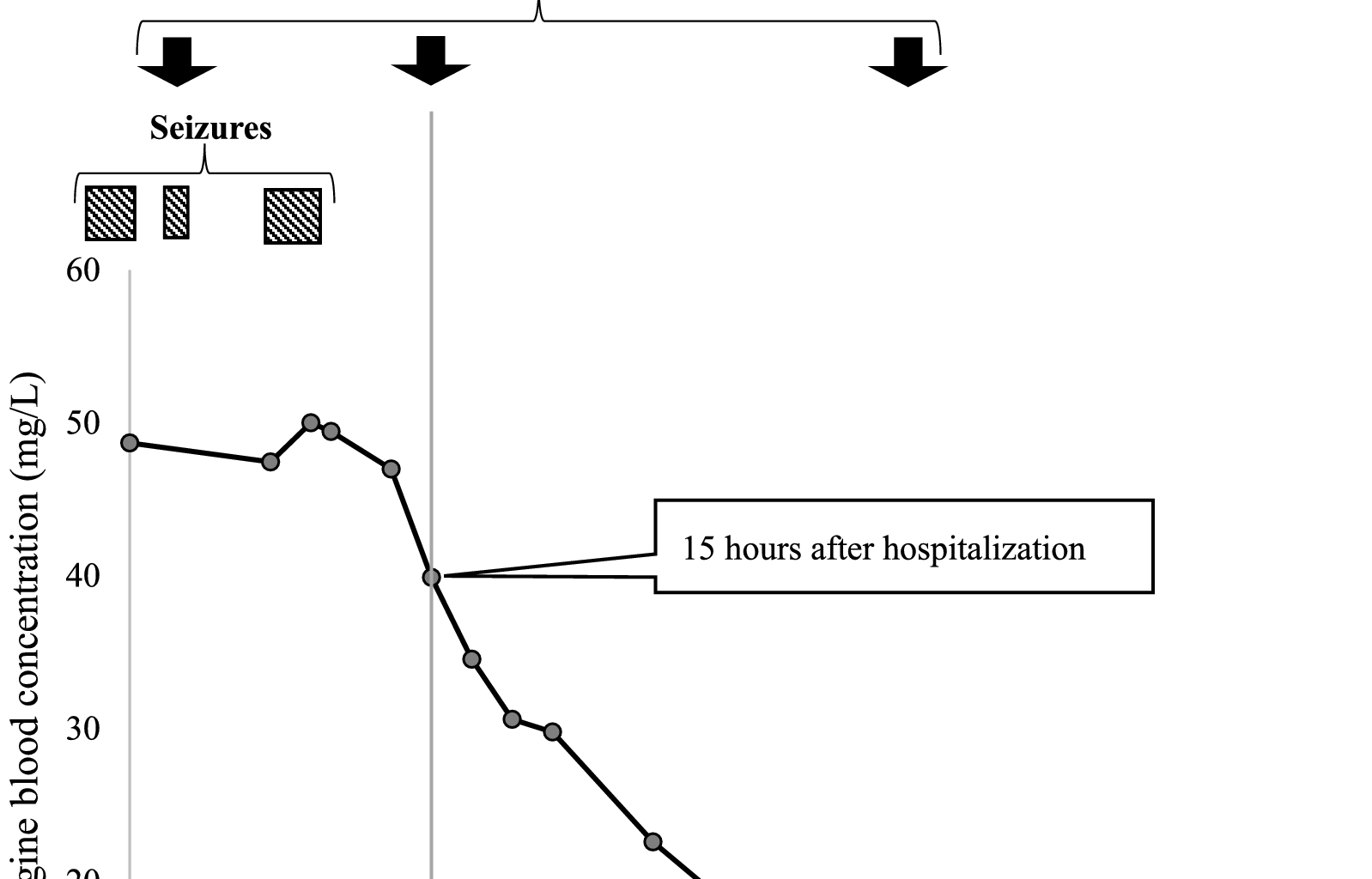
The concentration of lamotrigine in the blood notably decreased after 15 hours of hospitalization in this patient (Fig. 1). The pharmacokinetics of lamotrigine can be explained using a one-compartment model [10], and lamotrigine exhibits linear kinetics even after overdose [11], suggesting that the excretion rate changes after 15 hours. Fosphenytoin may have played a role in the decrease in the blood concentration.
Fosphenytoin undergoes complete metabolism to phenytoin via phosphatases, which are abundant in tissues, with a conversion half-life of 7–15 minutes [12]. The peak serum total phenytoin concentration is typically reached within 1 hour of fosphenytoin administration [13]. Phenytoin then promotes glucuronidation, decreasing the blood concentration of lamotrigine. While the average half-life of lamotrigine in combination with drugs that promote glucuronidation is 13.5–15 hours [6], in this particular patient, the patient’s lamotrigine levels did not exhibit a 50% reduction 15 hours after the initial dose of fosphenytoin. This may be due to excessive lamotrigine ingestion and reabsorption through the enterohepatic circulation.
Drugs with enterohepatic circulation have multiple peak blood concentrations [14], and the increase in lamotrigine blood concentration from 7 to 9 hours after admission may be explained by enterohepatic circulation. Repeated administration of activated charcoal has been reported to suppress enterohepatic circulation of lamotrigine and shorten its half-life [15]; therefore, the repeated administration of activated charcoal should also be considered for the treatment of lamotrigine overdose.
To the best of our knowledge, no studies regarding the effects of midazolam, fat emulsion, levetiracetam, or thiopental on the blood levels of lamotrigine have been reported. Activated charcoal was administered 1 hour after admission in this patient, well before the blood lamotrigine levels began to decrease. Therefore, it is unlikely that the activated charcoal affected the blood concentration of lamotrigine in this patient.
Fosphenytoin is also recommended as an antiepileptic drug when benzodiazepines are ineffective [16]. In this patient, the administration of benzodiazepines failed to control the seizures, though they did stop after the first administration of fosphenytoin. Therefore, fosphenytoin can be considered an effective antiepileptic agent in the setting of lamotrigine overdose.
The concomitant use of lamotrigine and fosphenytoin has some limitations. Both lamotrigine and fosphenytoin exhibit sodium channel blocking effects. Therefore, their concomitant use may increase the risk of arrhythmias. In cases of lamotrigine overdose, the inhibition of sodium influx into myocytes during phase 0 of the myocardial action potential can lead to intraventricular conduction delays, manifesting as prolongation of the QRS and corrected QT intervals on electrocardiography, as well as an increase in the R wave amplitude exceeding 3 mm in the lead aVR [17, 18]. This may account for the TdP that developed in the current patient. Sodium bicarbonate administration for these arrhythmias is thought to decrease drug ionization and reduce cardiotoxicity [19]. In this patient, QTc prolongation and R-wave elevation in the aVR lead improved after sodium bicarbonate administration, and fosphenytoin administration did not lead to arrhythmia. Therefore, the absence of ECG abnormalities should be confirmed before the administration of fosphenytoin.
Fosphenytoin has the potential to shorten the half-life of lamotrigine and also exerts antiepileptic effects in patients experiencing a lamotrigine overdose.