
Data
We used routine health insurance data of the statutory health insurance BARMER, covering approximately 8.7 million individuals (10.3% of the German population) within the study period 2020–2023. These data contained information on medical procedures coded according to the “Operationen- und Prozedurenschlüssel” (OPS; German modification of the International Classification of Procedures in Medicine) and inpatient and outpatient diagnoses coded according to the International Statistical Classification of Diseases and Related Health Problems, 10th Revision, German Modification (ICD-10-GM). The data also provided information on demographic characteristics, including date of birth, sex, and date of death.
Inclusion and exclusion criteria
We included hospital cases with TKA according to the definition underlying the official minimum volume regulation of the German Federal Join Committee (Gemeinsamer Bundesausschuss, G-BA)14. This definition was based on specific OPS codes within the group “5–822 Implantation of an endoprosthesis in the knee joint” (see supplementay material, Table S1 for details). We selected those TKA cases with date of surgery in the period 2020–2023. To ensure a homogeneous study population, we included only hospital cases with specific diseases coded as main diagnoses. These diseases included rheumatoid arthritis, soriatic and enteropathic arthropathies, juvenile arthritis, gonarthrosis, and osteonecrosis (ICD-10-GM codes are provided in the supplementary material, Table S2).
We followed the definition of exclusion criteria proposed by the AOK Research Institute (Wissenschaftliches Institut der AOK; WIdO)15 and excluded cases with specific procedures coded during the same hospital stay. These procedures included implantation of an endoprosthesis in the hip joint, implantation or replacement of a tumor endoprosthesis, implantation of a modular endoprosthesis or (partial) replacement in a modular endoprosthesis in bony defect situation and possible (partial) bone replacement, and implantation of or (partial) replacement to a custom-made implant in bony defect situation or congenital or acquired deformity. We further excluded patients with previous TKA within two years before the date of surgery. Since outcomes could not be observed (see below), we excluded patients who died or were not continuously insured within one year after TKA. To ensure that pre-existing comorbidities can be fully observed, we excluded patients who were not continuously insured for at least one year before TKA. For some TKA cases, hospital case volume could not be determined because hospitals not further aiming to provide TKA were not required to retrospectively report hospital case volumes to the G-BA. Those cases were also removed from our analysis. Finally, demographic characteristics like age were not available for specially protected groups of persons. Corresponding hospital cases were also excluded.
Outcomes
We considered two outcomes, which have been frequently employed in related studies1. First, we observed for each included TKA case whether there was revision TKA within one year after the date of surgery. Second, we considered surgical complications within one year after the date of surgery. Such complications included fracture of bones, dislocations of the knee, disruption of operation wounds, infections, and inflammatory reactions. The operationalization of both revision TKA and surgical complications followed the AOK research institute15 (OPS and ICD-10-GM-codes are provided in the supplementary material, Tables S3 and S4).
Death within one year after surgery was used as exclusion criterion to ensure that revision TKAs and surgical complications could be fully observed. However, mortality itself is a potential—although very rare—outcome associated with TKA16. We therefore investigated the relationship between hospital case volume and 90-days mortality for sensitivity analysis.
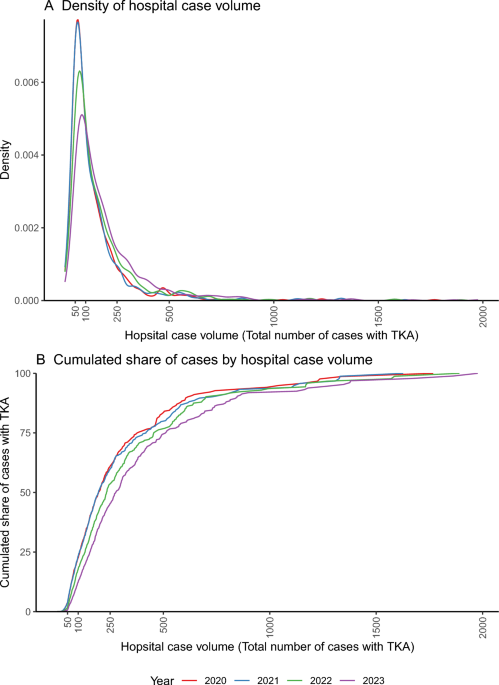
Hospital case volume
Hospital case volume was defined as the yearly number of cases with TKA treated in a specific hospital. Data on hospital case volume was derived from the “minimum volume data” provided by Verband der Ersatzkassen (vdek). Retrospective reporting of these data was obligatory for all hospitals aiming to offer TKA since the introduction of a minimum volume standard.
Given these data, we explored two different approaches of modeling volume-outcome relationships: In our main analysis, we investigated associations between patient outcomes and contemporary hospital case volume, i.e. the number of cases with TKA the hospital treated in the year of the patient’s surgery. For sensitivity analysis, we used the hospital’s average number of TKA cases within the three years preceding the year of the patient’s surgery. The latter approach reflects the conjecture that potential effects of learning-by-doing17 may be better captured by historical than by contemporary treatment volumes.
Covariates
To adjust for patient-specific risk factors, we utilized information on the patients’ sex and age at the date of TKA. Since obesity was found to be a main risk factor for adverse outcomes after TKA18,19, we included body mass index (BMI) categories of 30- < 35, 35- < 40, and 40 + in our models. We further included all Elixhauser comorbidities20 except for obesity as separate indicator variables. We also adjusted for osteoporosis if it was coded during the hospital stay when the patient was undergoing TKA. Potential time effects were captured by dummy variables for the years 2021–2023, where the year 2020 served as reference category.
Statistical modeling
We applied logistic regression to model associations between patient outcomes, hospital case volume, and covariates. For flexible modeling of such associations, we used natural cubic splines of hospital case volume13. Natural cubic splines facilitate the identification of nonlinear relationships by fitting piecewise polynomials to the data. Such splines may be specified with different degrees of freedom, which determine the flexibility of the estimated relationship. While one degree of freedom is equivalent to including hospital case volume without any transformation to the regression model, two degrees of freedom correspond to two fitted piecewise polynomials (and, consequently, one knot connecting these polynomials), three degrees of freedom correspond to three fitted piecewise polynomials, and so on. To find the most accurate specification, we estimated models including splines with one to ten degrees of freedom. We then applied the Akaike information criterion (AIC)21 to select the model with the best fit to the data. To account for correlation of patient outcomes within hospitals, we applied clustered standard error estimators.
Given the model selected according to the AIC criterion, we derived predicted outcome probabilities with 95%-prediction intervals (95%-PIs) conditional on hospital case volume for a representative patient. A representative patient was defined as a patient with average values of all covariates (e.g. average age and average prevalence of comorbidities).
For sensitivity analysis, we applied generalized additive mixed models (GAMMs) with smoothing splines as an alternative modeling approach22,23.
Ethics
The ethics committee of the North Rhine State Chamber of Physicians (Ärztekammer Nordrhein; ÄkNo) waived the needs for ethics approval and informed consent for this study (reference number: 171/2024). This study adheres to all relevant regulations and guidelines, including the General Data Protection Regulation of the European Union, the Declaration of Helsinki, and the guidelines for good practice secondary data analysis (GPS) of the German Society for Epidemiology (DGEpi)24.