
Changes could touch 760,000 HMSA members and their doctors.

Getty Images
In mid-January lawmakers from the Hawaiʻi House and Senate committees on consumer protection called in executives from HMSA and Hawaiʻi Pacific Health to explain their proposal to create a new system designed to address Hawaiʻi’s health care crisis.
Despite lengthy talk about “risk-sharing,” “value-based care” and “bending the cost curve,” the presentation by Hawaiʻi Pacific Health’s chief executive, Ray Vara, and his HMSA counterpart, Dr. Mark Mugiishi, left some lawmakers with more questions than answers.
“It’s been a real challenge to understand,” said Sen. Jarrett Keohokalole, a lawyer accustomed to parsing minutiae as chair of the Senate Commerce and Consumer Protection Committee.
Keohokalole isn’t alone. Doctors have also raised concerns, citing a lack of details about the proposal. And The Queen’s Health Systems has said the deal could pose a threat to its existence.
The deal, which would bring together the state’s largest health insurer and one of its biggest hospital companies under a new umbrella organization called One Health, is likely to touch the lives of some 760,000 Hawaiʻi residents and their doctors.
 Hawaiʻi Pacific Health, one of the state’s largest health providers, is planning a deal with HMSA, the state’s largest health insurer. (Cory Lum/Civil Beat/2019)
Hawaiʻi Pacific Health, one of the state’s largest health providers, is planning a deal with HMSA, the state’s largest health insurer. (Cory Lum/Civil Beat/2019)
Vara and Mugiishi’s main talking points are clear and reassuring to the general public: HMSA members will still be able to choose their own doctors, and the rate of rising insurance premiums will go down along with overall health care costs.
Still, by Vara’s account, the proposed deal represents a major “180-degree turn in the way health care is delivered and funded.” Proponents like Vara and Mugiishi say their plan is the best way to squelch rising health care costs and insurance premiums while promoting better outcomes for patients.
The alternative, Vara and Mugiishi say, is a system that’s inexorably breaking down. Merely tweaking the system amounts to making stop-gap gap repairs to a car that’s falling apart. Hawaiʻi, they said in a wide-ranging interview, needs a new car.
“The system is not only ripe for change,” Vara said, “but the system itself is unsustainable.”
The proposal comes as Hawaiʻi’s dominant health insurer is struggling. And so are health care providers.
In 2025, for the first time in nearly 20 years, Hawaiʻi Pacific Health, a nonprofit that owns Kapiʻolani Medical Center for Women and Children, Pali Momi Medical Center, Straub Medical Center, Wilcox Medical Center and numerous clinics, posted an operating loss, Vara said. In fact, he said, every health system in Hawaiʻi lost money in 2025.
The situation at HMSA is also bad. According to its two most recent financial statements, Hawaiʻi’s largest health insurer has suffered escalating operating losses in recent years, even as premiums rise. The bottom line: medical claims are exceeding premiums, and the situation is getting worse.
HMSA suffered a $117.4 million operating loss in 2024, despite raking in $4.4 billion in member premiums. The only reason it has remained in the black the last two years is because of income from investments and other sources.
 Ray Vara, CEO of Hawaiʻi Pacific Health, and state Rep. Linda Ichiyama survey an area set up as a mass vaccination center in 2021. (Stewart Yerton/Civil Beat/2021)
Ray Vara, CEO of Hawaiʻi Pacific Health, and state Rep. Linda Ichiyama survey an area set up as a mass vaccination center in 2021. (Stewart Yerton/Civil Beat/2021)
 HMSA CEO Dr. Mark Mugiishi is one of the leading proponents of the proposed One Health deal. (Cory Lum/Civil Beat/2022)
HMSA CEO Dr. Mark Mugiishi is one of the leading proponents of the proposed One Health deal. (Cory Lum/Civil Beat/2022)
Consumers are starting to feel the existential financial stress the system faces. Self-employed workers and their families covered by Affordable Care Act plans on average saw a 26% premium increase for 2026.
Employed workers in Hawaiʻi have been somewhat insulated from premium increases by the state’s health care law, which requires employers to provide insurance for employees working 20 hours or more per week. Employers are feeling the cost, though, with the impacts rippling through the economy. And workers still experience trouble when it comes time to find a new primary care doctor or specialist.
Skeptics question the proposal, saying, among other things, that HMSA’s current risk-sharing model already has contributed to Hawaiʻi’s doctor shortage, which has diminished access to care for people throughout the state and especially on neighbor islands. Others say the deal will hurt the most vulnerable — sick, elderly and low-income patients — and the doctors and hospitals that treat them.
But the leaders behind the One Health proposal say the most harmful strategy would be to continue down the path Hawai‘i’s health system is on.
“And so while there may be fear of the unknown,” Vara said, “quite honestly, I think the greater fear should be of the known: what we’re currently experiencing.”
A Trust Problem
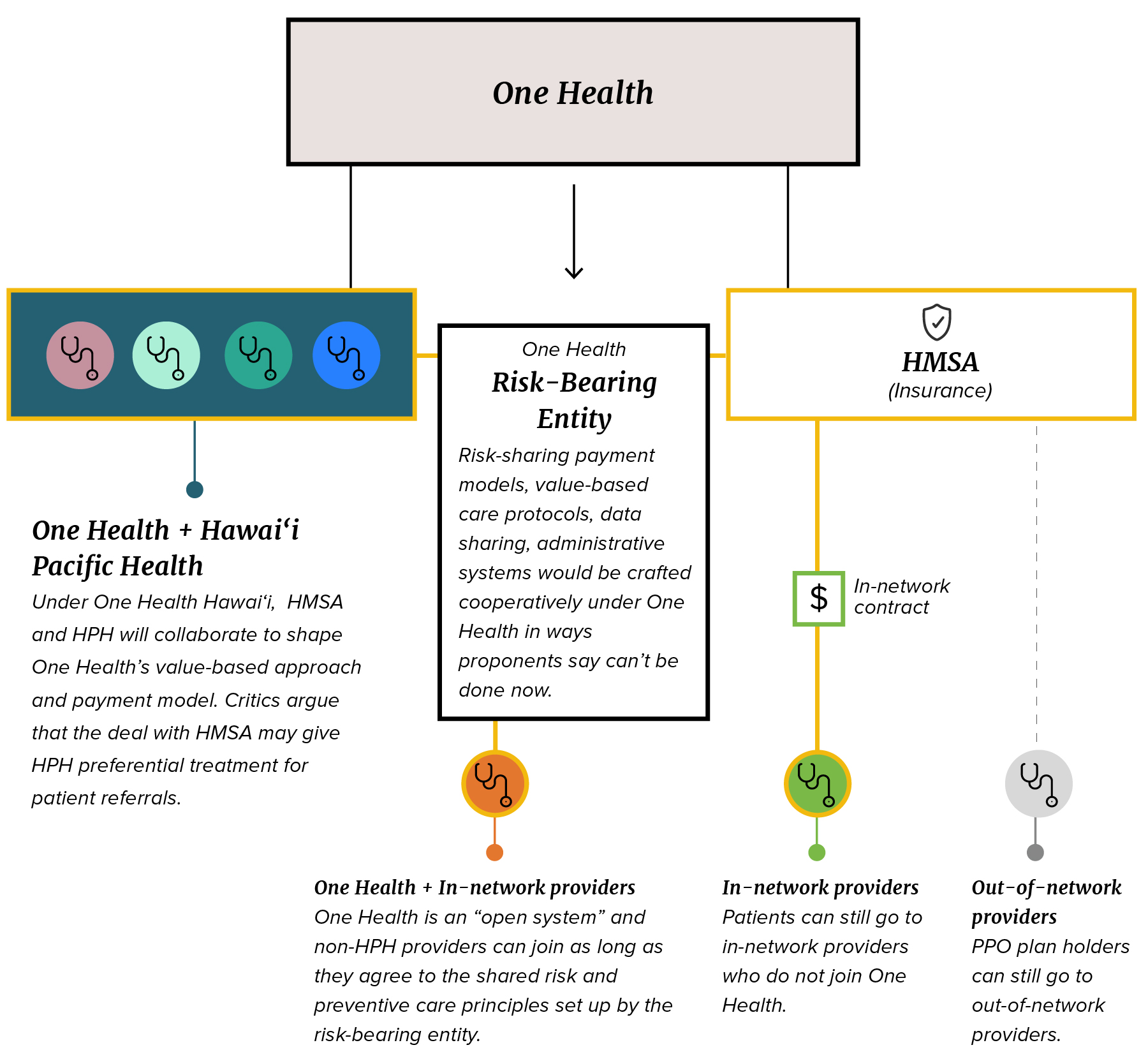
One Health’s proponents say consumers wouldn’t likely see much change, if any. Their HMSA health plan would still allow them to see anyone in the HMSA network, which would be separate from One Health.
However, the One Health proposal could radically change the health care system, particularly the way insurers interact with doctors and hospitals.
The One Health proposal is not a merger — HMSA and HPH will continue as separate entities but collaborate through what they call a “risk-bearing entity.” HMSA members should be able to keep seeing the doctors they want, but to be part of HMSA’s network, doctors outside of HPH will have to continue to negotiate separate contracts with HMSA.Other doctors and hospitals will be able to join One Health as long as they adopt its policies for sharing risk and caring for patients.Some believe Hawaiʻi’s neediest residents could lose access to critical health care if the deal goes through.
Under a model people are most familiar with, insurance companies bear all of the risk: a sick patient goes to the doctor, the doctor treats the patient and then gets reimbursed by the insurer – something known as “fee for service.” If the doctor ends up with a lot of sick patients who need a lot of care, it falls onto the insurers.
Over the past decade, HMSA has moved away from that payment system for primary care doctors. Under the current system, HMSA negotiates multi-year contracts with physicians, who are typically represented by physician organizations. Central to these contracts are so-called risk-sharing payment models.
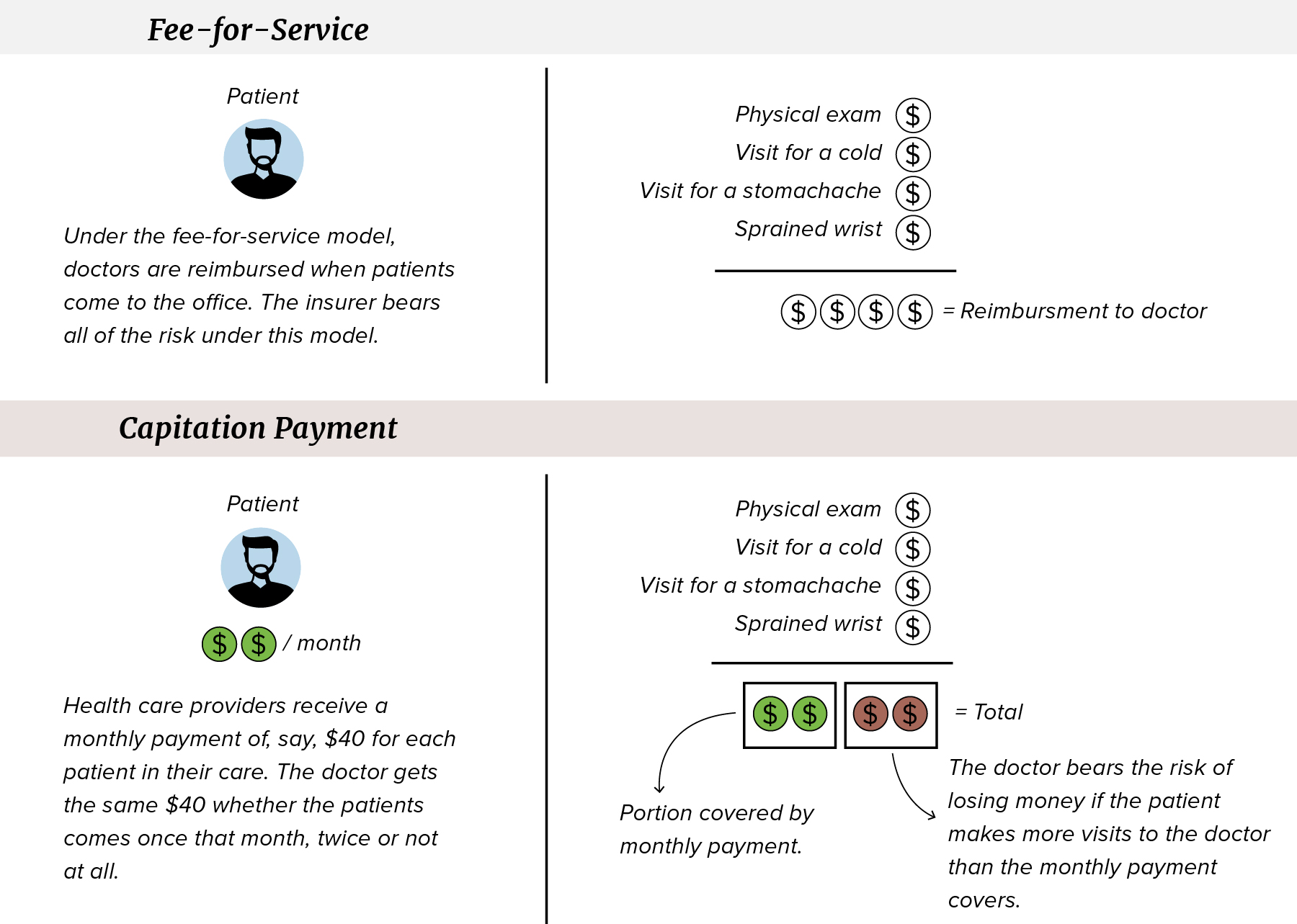 The proposal calls for moving doctors to what is known as a capitation system. (April Estrellon/Civil Beat/2026)
The proposal calls for moving doctors to what is known as a capitation system. (April Estrellon/Civil Beat/2026)
With HMSA’s risk-sharing payment model, primary care doctors in HMSA’s commercial insurance network generally aren’t paid a fee each time they see a patient. Instead, HMSA pays primary care doctors what amounts to a monthly allowance per patient, called capitation in medical parlance.
Primary care doctors generally get about $40 per month per patient. To break even or make a profit, the doctors need 1,000 to 2,000 people under their care, so the healthy ones needing fewer visits can make up for sicker or older ones who need more visits.
Related to risk-sharing are care protocols, which health care professionals call “value-based care.” The concept is based on the adage that an ounce of prevention is worth a pound of cure. Doctors provide preventative care, patients stay healthy and HMSA doesn’t have to pay for higher-cost procedures later.
The challenge is creating a system to account for the ounces of prevention doctors are doling out. To do that, HMSA relies on quality metrics. Doctors can get much-needed bonuses for meeting HMSA’s quality metric goals.
The current quality metric system adds costs for everyone. Insurers need costly technology and staff to track whether the doctors are meeting their quality metrics. Doctors need to submit extra paperwork to the insurer, adding what many doctors say is an enormous administrative burden.
Vara and Mugiishi say One Health would dramatically change that model. Risk-sharing and value-based care would remain central components. In fact, the idea is to expand the allowance-based, risk-sharing payment model beyond primary care doctors to specialists and surgeons, something known as “global capitation.”
Value-based care would also be expanded beyond primary care doctors, who Mugiishi said, represent “a tiny fraction of the total health care spend.”
“Most of the spend comes from hospitals or specialists or pharmacy,” Mugiishi said in an interview. “None of those are in value-based care.”
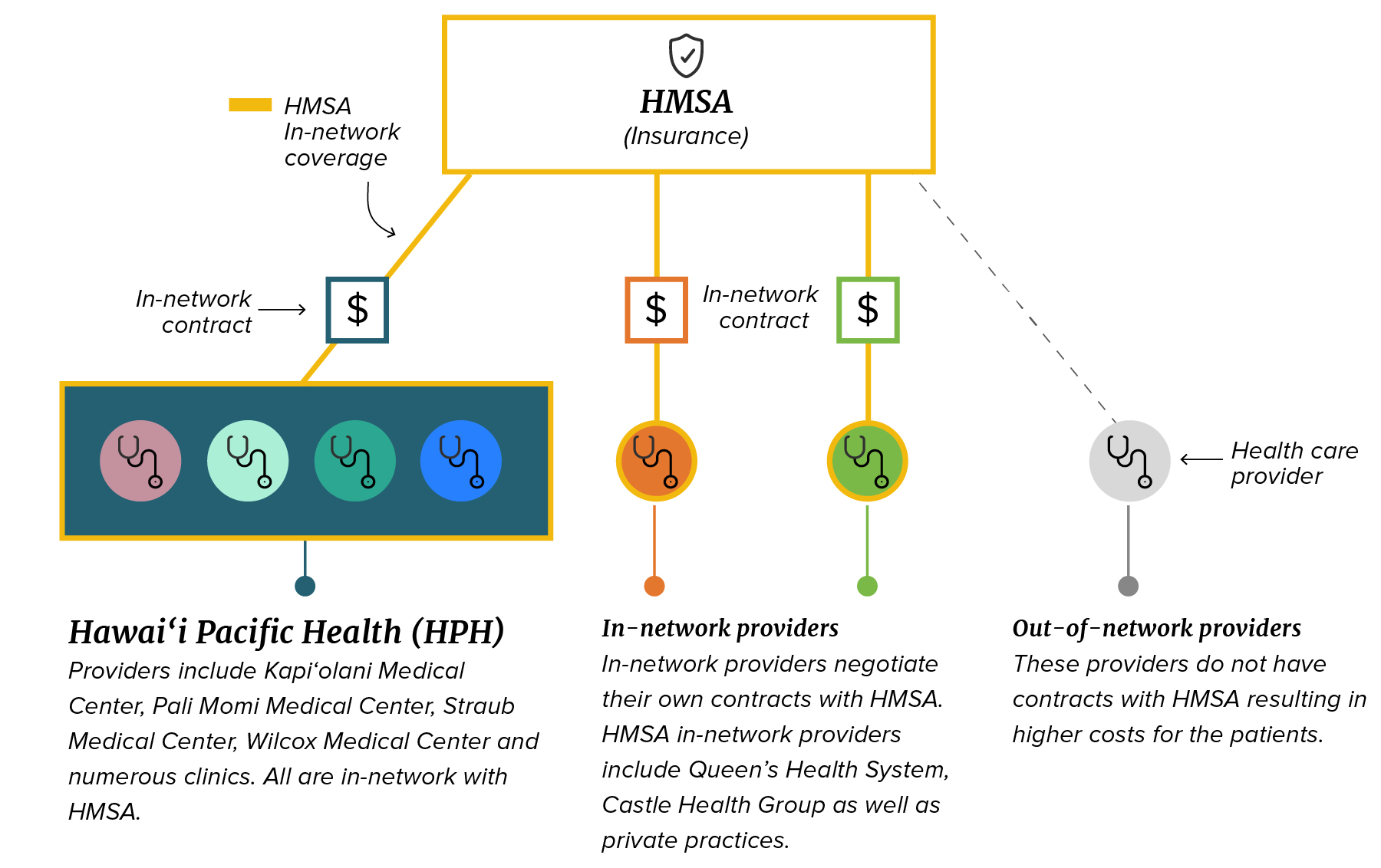 Under the current system, doctors and hospital groups negotiate contracts individually with insurance companies like HMSA. (April Estrellon/Civil Beat/2026)
Under the current system, doctors and hospital groups negotiate contracts individually with insurance companies like HMSA. (April Estrellon/Civil Beat/2026)
Central to One Health, Vara and Mugiishi said, is a planned data-sharing system designed to reduce the red tape doctors face when dealing with HMSA, dramatically lowering administrative costs for both sides.The system could also reduce the need for prior authorizations from HMSA.
Another cost-saving measure: what Vara calls “coordination of care,” which among other things, includes avoiding duplicating services and steering some outpatient surgeries from hospitals to less costly ambulatory surgical centers.
Though often described as a merger, the new system would be open to any doctor, physician group or hospital that agrees to the overarching ideas of risk-sharing and providing value-based care to lower costs with the goal of creating a healthier community. Vara said he understands that specific payment models might not work for every doctor or hospital. The idea would be to tweak contract terms between such providers and HMSA to account for that as long as the providers agreed to the overarching principles.
“Everybody will be able to latch on depending on where they’re at,” he said in an interview.
A main goal, Vara said, is to create more trust and cooperation between HMSA and the providers. Vara recognizes a natural tension between the two sides. At their core, insurers are financial institutions with duties to make sure money is paid out carefully. Providers, meanwhile, have a mission to treat people, and they want the insurers to pay for that treatment. It creates what Vara calls “a natural conflict between two very important stakeholders.”
Doctors and insurance companies are bound together by contracts but, Vara said, “Contracts can’t really buy trust.”
 The proposed deal brings together HMSA and HPH through a third entity that is meant to enable a different kind of health care delivery and payment model. (April Estrellon/Civil Beat/2026)
The proposed deal brings together HMSA and HPH through a third entity that is meant to enable a different kind of health care delivery and payment model. (April Estrellon/Civil Beat/2026)
Vara likens the current level of trust between insurers like HMSA and providers like Hawaiʻi Pacific Health to that of a dating couple. You wouldn’t share your bank account with someone you just started dating, but once you get married that usually changes.
The idea is that One Health can serve as a marriage between HMSA and Hawaiʻi Pacific Health that anyone else can join. Central to the marriage is what Vara calls a “risk-bearing entity” — a separate outfit created for One Health that will allow HMSA and HPH to share patient data and collaborate on policies and procedures that they can’t do through standard, arm’s-length contract negotiations. Any doctor or hospital would be able to bolt on to the entity as long as they agreed to follow the entity’s policies and procedures.
‘Risk-Sharing’ And ‘Value-Based Care’ Worry Doctors
Some doctors are not convinced. Particularly worrisome to some is HMSA’s monthly allowance payment model for primary care doctors, which could be expanded under One Health.
As HMSA’s Mugiishi sees it, primary care doctors have been satisfied with the monthly allowance model. He points to a 2024 survey conducted by HMSA that included 646 primary care doctors. It found 88% said the amount of time they get to spend with each patient has stayed the same or increased since HMSA adopted the monthly allowance system, and 75% said the system had made their practice financially the same or stronger.
But an independent study showed something very different.
A 2022 survey of Hawaiʻi physicians published in the Hawaiʻi Journal of Health and Social Welfare found that 77% of the 250 doctors who responded were unhappy with the payment model, with 55.2% reporting they were “very unhappy.” The study built on a previous, similar study that shared an overarching finding: that HMSA’s risk-sharing payment system was worsening Hawaiʻi’s physician shortage.
 Dr. Nadine Tenn Salle, president of the Hawaiʻi Medical Association, questions expanding a risk-sharing payment model that has left many primary care doctors unhappy. (Cory Lum/Civil Beat/2019)
Dr. Nadine Tenn Salle, president of the Hawaiʻi Medical Association, questions expanding a risk-sharing payment model that has left many primary care doctors unhappy. (Cory Lum/Civil Beat/2019)
Dr. Nadine Tenn Salle is a pediatrician who represents doctors as president of the Hawaiʻi Medical Association. In a statement, she said the organization hasn’t taken a position on the One Health deal. But she said HMSA’s monthly allowance-based model has led many physicians to “report increased administrative burden, uncompensated work, and rising stress — all of which have contributed to workforce strain.”
“If HMSA is now describing itself as being in a financially unsustainable position after years of operating under this model,” she added, “it raises an important question: why would we expand a model that has struggled in primary care to specialists and across the broader health system without first understanding what didn’t work and why?”
Meanwhile, for some doctors, “value-based care” translates simply to onerous administrative work.
Dr. Curtis Takemoto-Gentile cut ties with HMSA in January, opting to ditch insurance entirely and transition to a direct primary care model in which patients pay him $200 per month to be part of his practice, which he shares with his daughter, Dr. Krishanna Takemoto-Gentile.
 Dr. Curtis Takemoto-Gentile walks with his patient, Maureen Harnisch, in his Honolulu clinic. Takemoto-Gentile cut ties with HMSA in part because of the risk-sharing, value-based care model. (Kevin Fujii/Civil Beat/2026)
Dr. Curtis Takemoto-Gentile walks with his patient, Maureen Harnisch, in his Honolulu clinic. Takemoto-Gentile cut ties with HMSA in part because of the risk-sharing, value-based care model. (Kevin Fujii/Civil Beat/2026)
Dr. Curtis Takemoto-Gentile recalls when HMSA first started its monthly allowance payment model about eight years ago, the insurer paid him $45 per month. HMSA later cut that to $44. And he says he was relatively lucky: some doctors, he said, were paid as little as $18 per patient per month.
On top of the strict budget was the administrative burden of documenting that he was meeting HMSA’s quality metrics, something he says ate into nights and weekends. Making matters worse, Takemoto-Gentile says, he would have done all the things HMSA required him to do and document anyway.
“Why are we going through this paperwork to show that 80% of our patients got colonoscopies?”
Dr. Curtis Takemoto-Gentile
“Why are we going through this paperwork to show that 80% of our patients got colonoscopies, that 80% got mammograms, that 80% got flu shots?” he said.
Cutting ties with HMSA has freed him from the administrative tasks, giving him more time to spend with patients. He was recently able to make his first house call in years, which he says, “was life-saving for the patient.”
Takemoto-Gentile said he’s skeptical of the idea of spreading risk-sharing and value-based care more broadly across the health system. But he said there’s something equitable about applying the models to include surgeons and specialists.
That way, he joked, “everybody can bitch at the same time, not just the primary care docs.”
This Doctor Says One Health Payment Model Works
Among doctors not complaining about the model is Dr. Dawn Miura, who’s spent 35 years as a primary care doctor. For years, Miura was part of a three-doctor private practice. Although independent, Miura and her partners worked within Hawaiʻi Pacific Health’s physician group, Hawaii Health Partners, which Vara says has 1,700 providers.
When Miura was looking for a young doctor to take over her practice a few years ago, Miura couldn’t find any takers, so she strengthened her connection to Hawaiʻi Pacific Health by joining the Hawaiʻi Pacific Health Medical Group as an employed physician.
Even before joining the medical group, Miura says she benefited from being part of Hawaiʻi Health Partners. Like Takemoto-Gentile, Miura said she wasn’t a fan of HMSA’s quality metric system. It was such a hassle that Miura and her partners had to hire a full-time medical assistant to deal with the paperwork required to prove she was doing routine things like pap smears, which she said “are part of my DNA” to do.
When she ordered a pap smear, Miura said, it wasn’t enough that the gynecologist who did the test had billed the insurer and had been paid by HMSA. Miura had to go through additional hoops to prove the test had been done.
“You paid for the pap smear, dude, but you can’t tell that I did it?” she says, recalling dealing with HMSA. “And that’s counting against me?”
The result: “I have to pay someone to call the gynecologist to ask them to fax the pap smear, to upload the pap smear to a system that doesn’t always work very well and to manually enter the date of the pap smear and to attest on my behalf that I say this pap smear really got done.”
When negotiating with HMSA on behalf of Hawaiʻi Health Partners, Miura says, it was enormously helpful to “have Ray Vara walk in the room and say, ‘Let’s clean this up a bit.’”
It’s important, she said, to have people familiar with the business of health care negotiating on behalf of doctors who are generally busy “working 70 hours a week to care for the 1,500 to 2,000 patients they’re responsible for.”
There’s another feature of the Hawaiʻi Health Partners current contract with HMSA that Vara says bodes well for One Health. For the last several years, Vara said, Hawaiʻi Health Partners has been working with an allowance-based budget model for all doctors, including specialists, known as “global capitation.”
Under the model, HMSA agrees to a budgeted amount to pay Hawaiʻi Health Partners to deliver all of its medical services for a year. At the end of the year, the budgeted amounts are reconciled with actual amounts spent. If the providers go over budget, Hawaiʻi Health Partners is on the hook; if Hawaiʻi Health Partners can serve its patients, keeping them healthy while going under budget, Hawaiʻi Health Partners splits the savings with HMSA and distributes the rest to the doctors.
For the past four years, Vara says, Hawaiʻi Health Partners has come under budget.
The doctors and other practitioners who are part of Hawaiʻi Health Partners, Vara said, “are getting performance bonuses today, this month.”
Concerns That Most Vulnerable Will Lose Care Access
An overarching concern is that some patients will find it even harder to get treatments under the One Health model, particularly people who need high-cost, low-reimbursement treatments, including low-income, uninsured, Native Hawaiian and Pacific Islander patients.
Leaders at The Queen’s Health Systems, which includes its flagship The Queen’s Medical Center on Oʻahu, hospitals on Hawaiʻi island and Molokaʻi, and dozens of other facilities worry that One Health will siphon away higher-reimbursement procedures that Queen’s needs to cover services that it provides for the community at a loss.
 The Queen’s Health Systems’ CEO Jason Chang says the One Health model could undermine its ability to provide care for Hawaiʻi’s neediest residents. (Cory Lum/Civil Beat/2022)
The Queen’s Health Systems’ CEO Jason Chang says the One Health model could undermine its ability to provide care for Hawaiʻi’s neediest residents. (Cory Lum/Civil Beat/2022)
As an example, Queen’s chief executive Jason Chang points to Queen’s behavioral health services. Queen’s provides about 87% of Hawaiʻi’s behavioral health beds, he said, and it’s part of the system’s mission to serve the people of Hawaiʻi as envisioned by Queen Emma when she established the hospital.
Behavioral health is a money loser for Queen’s, Chang said, costing the system about $15 million annually. And it’s something that nobody else wants to offer. Queen’s makes up for the loss with revenue from what Chang calls “core services”: more complicated, higher-reimbursement areas like cardiology, orthopedics, neurology, oncology, cancer care and surgery.
These services, he says, are important for not just Queen’s, but all hospitals, including those owned by Hawaiʻi Pacific Health.
“I know that that’s important to them, because if you look at the new Straub, they’re not building a bigger emergency room, they’re not putting in behavioral health services. They’re not putting any more medical beds. They’re putting in more ORs, more cath labs for cardiology, neurology and more ICUs. And they’ve already made the investment in the cancer center.”
The bottom line, Chang says, is that Hawai‘i Pacific Health is investing in profitable medical lines and will need patients to pay for the investment. Chang points to patients needing cardiac treatment as an example. Currently, Queen’s and Straub are essentially in competition for referrals from doctors needing cardiac care for their patients.
“We’ve been able to compete for the cardiac based on our quality and our costs and our outcomes,” he says.
But if One Health participants are encouraged by the risk-bearing entity’s policies to steer cardiac patients to Straub, he says, “That’s not a fair market anymore.”
Queen’s could lose not just the patients it needs to maintain its heart center, Chang says, but also revenue it needs to support things like behavioral health services.
“I worry about physicians in the community starting to say that … ‘I can’t survive in private practice if I don’t move that way.”
Jason Chang, CEO, The Queen’s Health Systems
The concern is that over time, the state will see a “degradation of these services that are important to the fragile people in Hawai‘i.”
Meanwhile, Chang said, he’s concerned that more doctors will feel pressure to migrate to One Health’s risk-bearing entity, regardless of whether they really want to – leading to even more referrals to hospitals participating in the risk-bearing entity for high-reimbursement procedures.
“I worry about physicians in the community starting to say that, ‘Well, it’s actually more profitable for me, personally to move this way,’ or ‘I can’t survive in private practice if I don’t move that way,” Chang said.
Another risk: Medical students could be steered toward One Health rather than hospitals outside the system, like Queen’s, Kuakini and Castle hospitals.
“Any new grad can be told, wow, that’s way more attractive,” he said.
Vara has responded to the idea that the risk-bearing entity’s policies would disfavor Queen’s by saying Queen’s turned down an offer to participate near the outset, an assertion Chang has confirmed – although he says it was his predecessor, Jill Hoggard Green, who turned down the offer.
 Dr. Jack Lewin, who heads the Hawaiʻi Department of Health’s Planning and Development Agency, will have to approve the deal. (Courtesy of Stony Brook University)
Dr. Jack Lewin, who heads the Hawaiʻi Department of Health’s Planning and Development Agency, will have to approve the deal. (Courtesy of Stony Brook University)
“What we’ve constantly said back to HMSA is that we believe in taking risk, and we’ll take risk with you,” Chang said at a forum hosted by the Hawaiʻi Medical Association in December. But Chang said as Queen’s heard more about the model, leadership determined the risk the hospital system would need to take on under the One Health plan was potentially too great for Queen’s.
The deal still needs regulatory approval from the U.S. Department of Justice. At the state level, Dr. Jack Lewin, who heads the Hawaiʻi Department of Health’s Planning and Development Agency, will have to weigh in. Lewin declined to talk specifically about the One Health deal, which will come before him.
But, he said, generally that there’s nothing wrong with a capitated, monthly allowance per-patient payment model, as long as the payment is adequate to cover the doctors’ costs of doing business – which he said it generally doesn’t.
Nonetheless, he said, a lot of doctors just want a model where they can simply treat patients as needed and get paid.
“The older guard of my fellow physicians,” he said, “are going to say, ‘Pay us a fee for service and shut up.’”
“Hawaiʻi’s Changing Economy” is supported by a grant from the Hawaiʻi Community Foundation as part of its work to build equity for all through the CHANGE Framework.