

What makes small town healthcare different
Published March 19, 2026 03:00 AM PDT
When a 911 call comes in from the nursing home in Leonardville, Kansas (pop. 432), it is a half-hour drive to the only emergency room in Riley county, at Ascension Via Christi Hospital.
The ride in the back of the ambulance can be bumpy and loud. It can smell like diesel. And on a bad day, Josh Gering, the Assistant Director of the Riley County Emergency Management Services told Reuters, you can hear the siren.
Gering has been in small-town EMS for 16 years. He grew up in Kansas, married his high school sweetheart and after she finished law school they moved to the Kansas town of Manhattan, (pop. 54,700) to raise a family in a place he says feels like home. It’s not uncommon for Gering to run into someone he’s saved at the grocery store.
Nearly 90% of the land in the United States is rural and about one in five people, or some 60 million, live throughout it according to the U.S. Census. Data also show rural residents are older, have worse health outcomes and less health care access than their urban counterparts.
The health of rural residents
Rural communities have fewer doctors and many areas lack internet connections for telehealth. More rural residents are uninsured than in urban settings.
A chart compares rural and non‑rural medians across access to care, social welfare, population, and causes of death. Rural marks show lower access and higher rates of uninsured children, older adults, obesity, smoking, and deaths from firearms, heart disease, and suicide.
There are about 2,000 rural hospitals available to intervene in their health emergencies and over 40% operate at a loss, according to Michael Topchik, the executive director of the Chartis Center for Rural Health, a healthcare analytics and consulting firm. Risk of closure looms, especially for hospitals in the southern half of the U.S.
When rural hospitals close, Topchik says, “Old communities literally dry up and tumbleweeds go down Main Street.”
Rural hospitals at risk of closure
Rural hospitals in the South and Midwest are more likely to be at risk of closing. In Kansas there are 99 rural hospitals and nearly half are struggling to stay afloat.
A U.S. map made of colored circles shows the share of rural hospitals at risk of closure. Southern and Midwestern states have the highest risk, with Texas and Kansas showing large, dark circles indicating many hospitals and high vulnerability.
Note: Rhode Island and New Jersey do not have rural hospitals.
Source: Chartis Center for Rural Health
Rural areas also have a high reliance on Medicaid, relative to the size of their populations. Medicaid is the public program that provides insurance to more than 70 million poor children, pregnant women, seniors and people with disabilities.
The July 2025 budget reconciliation bill included nearly $1 trillion in federal Medicaid cuts that, along with other measures, are projected to leave about 10 million people uninsured by 2034, according to estimates from the non-partisan Congressional Budget Office.
White House spokesman Kush Desai said rural hospitals struggled with low utilization due to declining populations, and increased Medicaid spending in the past had not helped. He said the Trump administration’s $50 billion Rural Health Transformation Fund would “push states to adopt meaningful healthcare reform that can actually make rural hospitals economically viable again.”
To gain insight into the factors that make rural hospitals so vulnerable to closure, Reuters spoke with experts in health data analytics whose research covers risk modeling and reimbursement trends and healthcare professionals working in rural communities. We also visualized federal statistics to provide context on the current state of U.S. healthcare.
Four cartoon owls stand in front of an emergency‑room sign.
Kansas as case study
Ascension Via Christi Hospital in Manhattan, KS, is a general hospital, part of a national non-profit healthcare system. The hospital serves both the people of the city – home to Kansas State University – and the rural community beyond the city limits. It has 150 inpatient beds, which is considered sizeable compared to critical access hospitals in rural areas, which can maintain no more than 25 beds by law.
Farmers in Kansas grow soybeans and hay under the Midwest’s wide prairie sky. Corn fields line the roads on the way to Riley County’s small towns. There are smaller medical facilities some distance from Manhattan, though two have shut down in recent years. There is a small surgical hospital near Ascension Via Christi, but it does not have an emergency room.
The only emergency room in the county
In Riley county, which has the highest level of poverty in Kansas, Ascension Via Christi hospital is the only medical facility with an ER.
A map highlights Riley County, Kansas, showing the only local ER and nearby hospitals, with charts indicating high poverty and limited hospital beds.
Source: Sheps Center for Health Services Research; U.S. Census
Hospitals the size of Ascension Via Christi provide fewer services than larger hospitals in denser cities with big populations. To understand that distinction, Reuters looked at payment data from the Centers for Medicare & Medicaid Services (CMS).
Billing for Medicare procedures are a good, albeit imperfect, proxy for services, as 68 million Americans are on Medicare, the government health insurance program for people over 65 and others who qualify because of disability or certain medical conditions. As most beneficiaries are older, and in rural areas even more so, obstetrics is not captured.
As it happens, OB/Gyn services are often the first to be cut when funding doesn’t come through and that loss may be a harbinger of trouble, according to Topchik, “When you see OB shutter, you often times are seeing the shuttering of general surgery.”
Rural hospitals struggle to balance high fixed-costs required to provide broad coverage for emergencies with low patient volume, which limits revenue. Affording talent can be a challenge, according to Bob Copple, the retired president of Ascension Via Christi.
Paying the salary of a specialist can be out of reach, “You need about 150,000 people to support one vascular surgeon. We don’t have that.”
Revenue from patients by state
Higher revenue means large hospitals can afford to pay for high-end specialists and services. Rural hospitals have less financial cushion to absorb shocks.
A chart compares patient revenue: non‑rural hospitals bring in far more across states, while rural hospitals show much smaller revenues.
If services aren’t available at Ascension Via Christi, residents face a drive. Copple says folks who live south go to Wichita. To the west, Salina is an hour and ten minutes. Topeka is an hour east and people in need of a hospital to the north may have to cross the state line into Nebraska.
The distance to other hospitals
The drive to larger hospitals in Wichita and Kansas City takes about two hours.
A map shows the long distances from Riley County to larger hospitals in Wichita, Topeka, and Kansas City.
Source: Sheps Center for Health Services Research
For the sickest, sometimes that drive is by ambulance. Gering says the five EMS stations in the county fielded roughly 300 “interfacility transfers” in 2025, out of about 2,000 911 calls.
Patients are moved from Ascension Via Christi to larger hospitals because of advanced cardiac issues, severe trauma or critical problems during labor and delivery. Often times they go to other facilities in the Ascension network.
Three cartoon owls stand in front of an “EMERGENCY” sign.
Who pays?
“Rural” can be defined by population, road ruggedness or commuting distance to the nearest big city. How best to measure the financial health of rural hospitals? Many ways.
The finances of small community healthcare are tethered to myriad Medicare reimbursement classifications and their accompanying acronyms that have been accumulating since government health insurance programs were first established in the mid-1960s.
Presidents and policies
Truman promoted rural hospital construction. Obama expanded insurance coverage. U.S. Presidents traditionally introduce policies to support rural voters.
A timeline shows seven U.S. presidents associated with major rural‑health policies, from hospital construction in 1946 to a rural health transformation program in 2025.
There are Disproportionate Share Hospitals (DSH), Rural Referral Centers (RRC) and Critical Access Hospitals (CAH). The latter is what most rural hospitals fall under. Under Medicare, Critical Access Hospitals are reimbursed on a cost-basis.
There are hospitals that use the Prospective Payment System (PPS). For these, reimbursement is based on fixed, predetermined rates that do not account for the higher per-patient costs in small rural hospitals with low volume.
There are also Rural Emergency Hospitals (REH), a designation which arose after a wave of closures in 2020, and which allocates enhanced Medicare payments to facilities that shutter inpatient care and focus on outpatient.
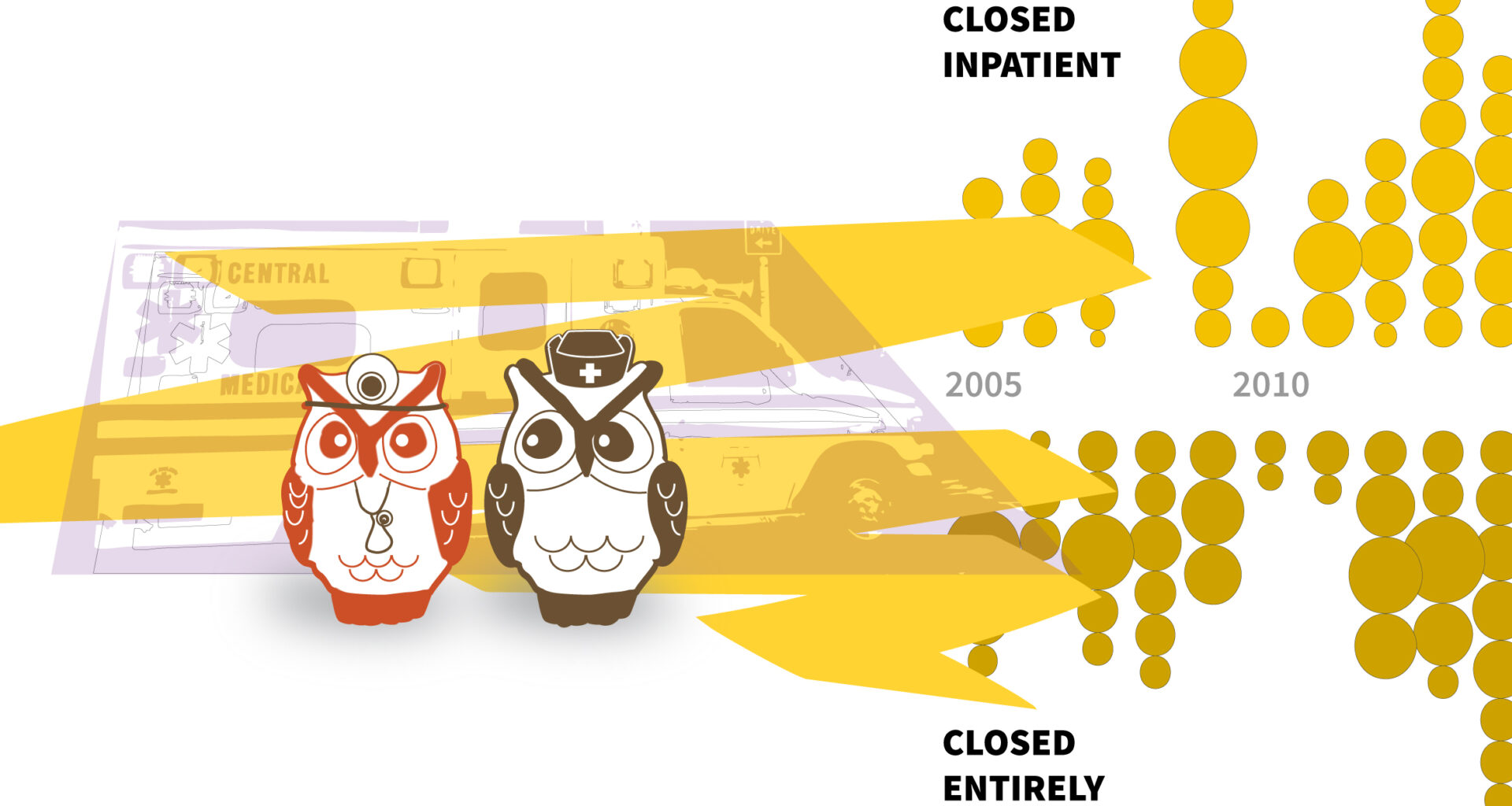
Losing beds or shutting down
Since 2005 more than 100 rural hospitals have closed and over 80 have shut down inpatient care.
A chart shows rural hospital closures since 2005, with many facilities shutting inpatient units or closing entirely.
Tyler Page is Deputy Director at the North Carolina Rural Health Research Program and an investigator with the Sheps Center for Health Services Research, a research institute at the University of North Carolina. He grew up in Farmer City, IL (pop. 2001).
The Sheps Center’s model looks at four sets of predictors with nearly 20 variables to determine the likelihood of distress in the next two years; Organizational traits like affiliation with a healthcare system, market characteristics, such as proximity to other large hospitals, financial performance and government reimbursement.
Page says rural hospitals are on a spectrum of financial vulnerability and it’s challenging to isolate the effect of one particular lever in a very complex box of levers. Both Page and Topchik told Reuters that one important predictor is the ratio of revenue from inpatient sources relative to outpatient.
Providing care, waiting for reimbursement
The percentage of outpatient charges (such as ER visits) or overnight stays (inpatient admissions) billed to Medicare reflects how state demographics strain rural hospitals. Further, hospitals with less billing are more likely to experience financial distress.
A scatterplot shows how states’ rural hospitals differ in the share of outpatient charges and inpatient admissions billed to Medicare, highlighting Southeast and Plains state patterns.
Data are median in each state as rates vary within states and state-by-state.
Source: Chartis Center for Rural Health
Most rural hospitals rely on outpatient care to stay afloat and have been shifting away from inpatient service which is more expensive.
Kirby Black is a rural emergency doctor and the medical director at the community hospital in Oneida, NY (pop. 10,666). Roughly 40% of his patients are on Medicaid. The hospital has about 30 beds staffed on any given day, a small OB unit and is on pace this year to lose $10 million from a $120 million budget.
Black says he misses when every encounter happened in a private room. Ten years ago, if he had a patient with chest pain who was low-risk, he would admit them overnight and run a stress test the next day. “Now I almost never admit patients for stress tests because I don’t have that space. We’re developing ways to do these as an outpatient instead of using an inpatient bed.”
Three cartoon owls stand in front of an illustrated emergency‑room backdrop in yellow and purple tones.
Politics at play
Medicare and Medicaid launched in 1966 as part of President Lyndon Johnson’s Great Society, amendments to Social Security to provide health insurance for older and low-income Americans who could not afford coverage.
States administered Medicaid. The Federal government provided matching funds. With more than 19 million Americans signing up for Medicare in the first year, the program provided a base of stable funding to fragile rural hospitals for the first time.
The Affordable Care Act (ACA) which President Barack Obama signed into law in 2010 was designed to expand Medicaid eligibility for low-income adults and provide health insurance marketplaces with government-subsidized private coverage. Forty states opted into expansion over a decade.
With a larger percentage of the population insured, Medicaid expansion drastically reduced the amount of uncompensated care and bad debt at rural hospitals, increased the amount of revenue and improved operating margins.
Who benefits?
Medicaid grew as the U.S. population grew, until health care reform under President Obama expanded the program and more adults joined the rolls.
A layered chart shows Medicaid enrollment growing across presidential administrations, with segments for elderly, adults, children, and disabled beneficiaries rising from Ford through Biden, and a marked jump during the Medicaid expansion era.
Source: Medicaid and CHIP Payment and Access Commission
The number of adults on Medicaid grew under the Affordable Care Act. When Obama first took office in 2009, roughly 60 million people were on Medicaid, one in four were adults. That number peaked at nearly 87 million in 2022, with the share of adults growing to 38%.
In states that adopted expansion, median Medicaid enrollment grew from roughly 15 to 21% of the total population. In rural areas with deep and persistent poverty, expansion was a stabilizing force for hospitals.
State Medicaid rolls before and after expansion
Expansion states saw substantial coverage gains in the percentages of Americans on Medicaid, regardless of whether the state leans Democrat or Republican.
Note: Medicaid recipients as a percentage of total state population
Source: U.S. Census Bureau
Republicans argue that the Affordable Care Act moved Medicaid too far from its original intent by loosening eligibility requirements, allowing able-bodied adults to join the rolls. Stricter conditions for maintaining benefits mandated by President Donald Trump’s Big Beautiful Bill, the budget spending bill that passed in Trump’s first year, go into effect Jan. 2027, two months after mid-term elections.
Nationally, the median operating margin for rural hospitals is 1.0%, according to Chartis, and within 16 states that margin is negative. Any loss in payments would erode margins that are already thin or non-existent.
Critics contend that growth in government appropriations mandated by law to provide health insurance, income or food assistance have shifted too much of the burden onto States.
Medicaid’s cut of state spending
States with high rates of uninsured and significant poverty spend a large percentage of their budget on Medicaid, which is jointly funded by states and the federal government.
A grid of pie charts shows how much each state spends on Medicaid, grouped by spending ranges. States with higher uninsured and poverty levels devote larger budget shares, with colors indicating political lean and non‑expansion status.
Source: National Association of State Budget Officers, 2023 FY
Harold Miller, the president of the Center for Healthcare Quality and Payment Reform, a national healthcare policy center, says being in an expansion state or reversing Medicaid cuts will not save small rural hospitals.
Miller says losses are also coming from private insurers and noted that Medicare Advantage will comprise 50% of rural patients by next year. Medicare Advantage plans are run by private insurers under contract with Centers for Medicare and Medicaid Services and are not required to reimburse Critical Access Hospitals on a cost-basis, unlike traditional Medicare.
He says many rural hospitals are out of network and “Medicare Advantage denies payment at an unusually high rate for small rural hospitals because small rural hospitals can’t fight back.”
The political landscape
Southern and central states have the largest number of rural hospitals, are more likely to vote Republican, and less likely to expand Medicaid.
A grid of colored circles arranged in a U.S. map layout shows the number of rural hospitals by state, with larger circles indicating more hospitals. Colors show states’ 2024 voting lean and whether they adopted Medicaid expansion. Southern and central states have the most rural hospitals.
Source: Chartis Center for Rural Health
Being an expansion state is one of the indicators data scientists at Chartis see in their vulnerability index as a protective factor. Their most recent modeling shows 417 rural hospitals are vulnerable to closure.
Beyond Medicare and Medicaid payments, rural healthcare providers also draw on county or city tax support, contributions from foundations or philanthropy, and regional corporate donors to stay afloat.
Riley county ambulance crews were able to use COVID funds to build a new headquarters. To celebrate, last June they opened the ambulance bay doors, bought snacks and a big frosted cookie with the star of life on it and invited the community.
Three cardiac arrest survivors showed up to thank Gering for saving their lives.
Three cartoon owls stand in front of an illustrated emergency‑room backdrop in yellow and purple tones.

Chartis Center for Rural Health vulnerability measure includes case mix index, government control status, average daily census swing/skilled nursing facility, average age of plant, average length of stay, occupancy, percent change in net patient revenue, years negative operating margin, Medicaid expansion status (state level), and traditional Medicare percentage days. Rural hospitals are facilities designated as a Critical Access Hospital or rural and community hospitals located in zip codes designated “rural” by the Federal Office of Rural Health Policy (FORHP) with no more than 200 beds; In Patient Revenue rural hospital is defined as any non-Native American/non-specialty facility with <200 beds located within an FORHP rural census tract: The North Carolina Rural Health Research Program mapping data includes Critical Access Hospitals, Rural Emergency Hospitals, and short-term, general acute, non-federal hospitals located in any non-metro county, metro census tracts with RUCA codes 4-10, or large area Metro census tracts of at least 400 sq. miles in area with population density of 35 or less per sq. mile with RUCA codes 2-3: Centers for Medicare and Medicaid Services Inpatient by Geography dataset contains hospital-specific charges for the more than 3,000 U.S. hospitals that receive Medicare Inpatient Prospective Payment System Part A Fee-For-Service for 523 services. Procedures combined to collapse levels of complications, RUCA codes for metro and rural only: National Association of State Budget Officers Medicaid spending amounts exclude administrative costs, include spending from state funds, federal matching funds and other funds used as a Medicaid match and Medicare Part D clawback payments. Medicaid beneficiary data exclude ‘other’ category.
Claudia K. Parsons, Matthew Weber