
Spinal deformities are prevalent in 84.0% of SMA patients, and 82.1% experience joint deformities or restricted joint mobility. The incidence of complications varies significantly among SMA subtypes, as detailed in Table 3. Specifically, the prevalence of swallowing/eating difficulties is significantly higher in type 1 and type 2 patients compared to type 3 patients (27.3% and 27.9% vs. 7.7%, P = 0.018). Similarly, respiratory difficulties are more common in type 1 and type 2 patients than in type 3 patients (45.5% and 34.9% vs. 13.5%, P = 0.011).
Table 3 . Factors influencing willingness to have another child
Spinal deformities are observed across all SMA types, with the highest incidence in type 2 patients (90.9% in type 1, 97.7% in type 2, and 71.2% in type 3, P < 0.001). Joint deformities or restricted joint mobility are also more frequent in type 2 patients compared to type 1 and type 3 (97.7% vs. 81.8% and 69.2%, P < 0.001). Despite the high prevalence of spinal deformities, 69.7% of affected patients have not undergone spinal surgery and do not plan to pursue surgical treatment. Additional complications reported include stomach pain, lower back pain, and osteoporosis. The results of multivariate analysis showed that male patients were less likely to develop spinal deformities than female patients (OR: 0.153; 95% CI: 0.038–0.620; P = 0.009). A higher educational level was associated with a lower prevalence of spinal deformity compared to a low education level (OR: 0.108; 95% CI: 0.030–0.387; P = 0.001) (Table 4).
Table 4 Factors influencing spinal deformity and motor functionMotor function
Analysis of motor function attained in the past revealed that the largest proportion of patients (42.5%) were able to sit independently. Significant differences in past motor function between patients with different subtypes of SMA (P < 0.001). Specifically, 72.7% of type 1 patients achieved the ability to sit with support, 37.2% of type 2 patients were able to sit independently, and a notable 80.4% of type 3 patients were able to walk independently without assistance. Whether or not the patient used DMT had a significant effect on past motor function (P = 0.026). Among those who have used DMTs, 48.6% were able to walk independently, compared to 28.1% of non-DMT users (Supplementary Table 1).
In terms of current motor function, there was a significant difference between patients who used and did not use DMT (P = 0.034). Specifically, 28.4% of DMT users are currently able to walk independently, compared to only 15.6% of non-users. Further stratification of SMA subtypes showed that there were also significant differences in current motor function between the different SMA subtypes (P < 0.001). Currently, 45.5% of type 1 patients cannot sit, while 27.9% of type 2 patients and 1.9% of type 3 patients fall into this category. Notably, 50.0% of type 3 patients are able to walk independently, whereas this ability is absent in type 1 and type 2 patients (Supplementary Table 2).
The results of multivariate analysis further showed that female patients had worse motor function than male patients (OR: 3.175; 95% CI: 1.131–8.907; P = 0.028). Patients with poor motor function have a lower level of education compared to patients with good motor function (OR: 12.067; 95% CI: 4.363–33.370; P < 0.001) (Table 4).
Main points of treatment in SMA patientsTreatment pattern
A total of 66.0% (70/106) of patients have received treatment with the intrathecal injection of nusinersen, and 24.5% (26/106) have received the oral solution of risdiplam. Notably, 20.8% (22/106) of patients have used both nusinersen and risdiplam. A smaller subset, 8.5% (9/106), have received non-DMT medications in the past or present, including drugs Like salbutamol, while 20.8% (22/106) have not received any SMA medication treatment. Medication usage among different SMA subtypes is depicted in Fig. 2, showing the highest proportion of patients using nusinersen across types 1, 2, and 3 (72.7%, 58.1%, and 71.2%, respectively). The decision to forego DMT treatment among SMA patients is primarily influenced by the high cost of drugs (88.9%), the inconvenience of treatment (44.4%), and uncertainty regarding the timing of treatment (22.2%). Among the 22 patients who have not received any SMA medication treatment, the most cited reasons were similarly high drug prices (81.8%), inconvenient treatment regimens (50.0%), and uncertainty about when to begin treatment (22.7%).
Fig. 2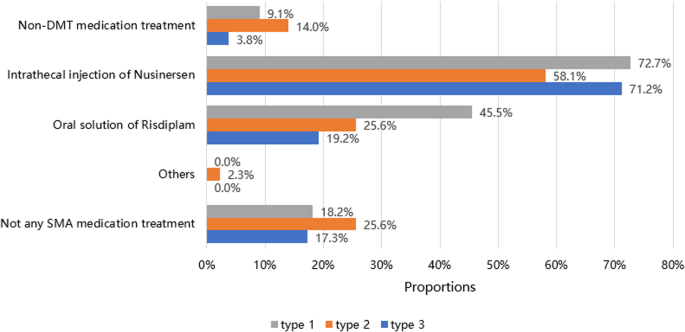
Past and current medication treatment status of SMA patients. DMT, disease-modifying therapy
Moreover, the study found that 81.7% of patients have not changed their treatment medication during the course of their treatment, whereas 18.3% have changed medication one or more times. The primary reasons for changing medications included lack of efficacy (41.2%), inconvenience of the treatment method (41.2%), and the pursuit of greater benefits (35.3%).
DMT medication
The age of initiation and duration of DMT also varied. The median age for starting risdiplam treatment was lower than that for nusinersen [14.50 (11.25, 18.75) vs. 16.50 (11.25, 25.75)], with 65.4% of risdiplam users having been on treatment for less than six months. In contrast, the majority of nusinersen users (74.3%) had a treatment duration of one to three years. Furthermore, the median age of initiation of nusinersen treatment was significantly younger in type 1 patients compared to type 2 and type 3 patients [10.50 (5.00, 11.00) vs. 16.00 (12.00, 24.00) vs. 20.00 (14.00, 28.00), P = 0.004].
Medication selection considerations
When selecting medications, the primary considerations among all patients included drug efficacy, safety, and cost (Fig. 3). However, 71.7% of patients reported a lack of clear understanding of the medication’s efficacy, and 51.9% were uncertain about the duration of treatment and which medication was suitable for them. Specifically, type 1 patients prioritized drug efficacy, severity of their condition, and safety; type 2 patients focused on efficacy, safety, and doctor’s recommendation; and type 3 patients considered efficacy, cost, and insurance coverage. For patients using DMT medications, the main factors were drug efficacy, insurance coverage, and safety, whereas those not using DMTs were more influenced by efficacy, doctor’s recommendation, safety, and insurance coverage.
Fig. 3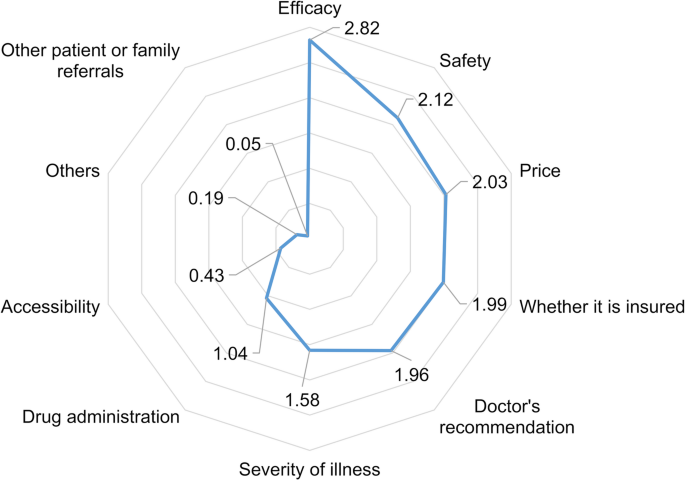
Ranking of factors considered when choosing different treatment medications. Note: The calculation formula for the weighted comprehensive score is: (Frequency of first place × 5) + (Frequency of second place × 4) + (Frequency of third place × 3) + (Frequency of fourth place × 2) + (Frequency of fifth place × 1)/total number of responses. For example, the comprehensive score for “Doctor’s recommendation” is calculated as (29 × 5) + (5 × 4) + (6 × 3) + (8 × 2) + (9 × 1)/106 = 1.96. The same method is used for calculating the comprehensive scores for other indicators
Treatment satisfaction
Regarding the current treatment received, 51.2% of the patients were satisfied, while 48.8% expressed some dissatisfaction, which was primarily attributed to the poor efficacy of the medication, lack of significant symptom improvement, and high treatment costs that impose financial strain on their families.
For SMA treatment medications, the efficacy outcomes that patients most commonly recognized included delaying disease progression, improving disease symptoms, and enhancing quality of life (Fig. 4). Differences were observed in the recognized outcomes among patients with different types of SMA. Improvement in disease symptoms was noted primarily in terms of overall mood enhancement (46.0%), motor function improvement (23.0%), and reduction in hospitalization rates (23.0%). Notably, type 3 patients (53.3%) and patients who have used DMTs (55.6%) reported more significant improvements in overall mood. Quality of life improvements were mainly characterized by enhancements in psychological and emotional status (36.2%) and physiological function (26.1%), among other factors.
Fig. 4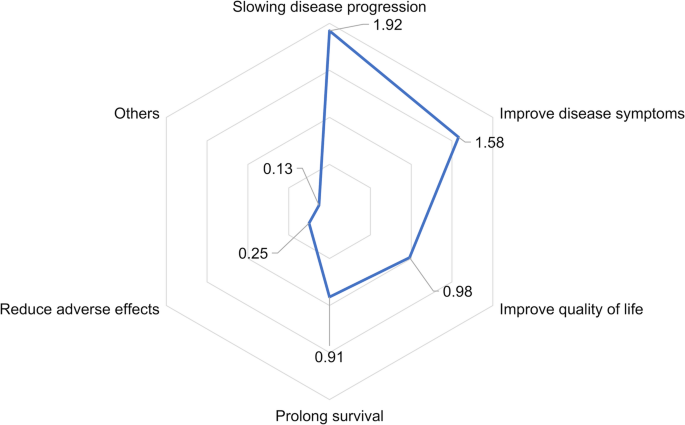
Ranking of recognized efficacy outcomes when choosing treatment medications
Route of administration and follow-up frequency
Notably, 70.8% of patients preferred solely oral medication therapy. This preference was consistent across patients with type 1, type 2, and type 3 SMA. Besides, the proportion of patients opting for oral treatment alone was significantly higher among those who had not used DMTs compared to those who had used DMTs (87.5% vs. 63.5%, P = 0.013).
In the past year, 50.0% of patients had more than three hospital follow-up visits, with type 3 patients exhibiting a higher follow-up rate than type 1 and type 2 patients. The proportion of patients with more than three follow-up visits was significantly greater among DMT users compared to non-users (72.1% vs. 3.1%, P < 0.001). Conversely, among patients who had not used DMT medications, 96.9% did not have any follow-up visits in the past year. The primary reasons for this lack of follow-up were high medication costs (69.4%), the inconvenience of treatment (55.6%), and perceived poor efficacy of medication (22.2%). Additionally, some patients cited the absence of an effective treatment plan or concerns about contracting cross-infections at the hospital as reasons for not attending follow-up visits.