
In examples like this across the United States, too many health care markets aren’t working. Markets are supposed to discipline prices. In a functioning, competitive market, a health care provider shouldn’t be able to charge twice as much for the same service and get customers. But in many parts of American medicine, markets fail to tame excessive prices.
For decades, American health policy has rested on a simple assumption: If there is enough competition, prices will fall. In the last two pieces of this series, we’ve laid out how regulators and policy makers have failed to foster adequate competition in some communities and what they can do to bring it back. But beyond making markets work, there are other options, especially when policy makers find that breaking up large systems which are behaving badly may not be tenable. When prices stop reflecting value and instead reflect leverage, there is another approach that much of the world uses: price regulation.
Americans often recoil at the idea of price regulation, seeing it as heavy-handed or anti-market. But health care prices are already regulated. Medicare sets payment rates for seniors. Medicaid does the same for lower-income Americans. Several states, such as Vermont and Indiana, recently enacted legislation to cap or freeze hospital prices for commercially insured patients. The real question isn’t whether prices can be regulated — they clearly can. It’s why we continue to allow American families in noncompetitive markets to be subjected to a system in which prices reflect market power, not value..
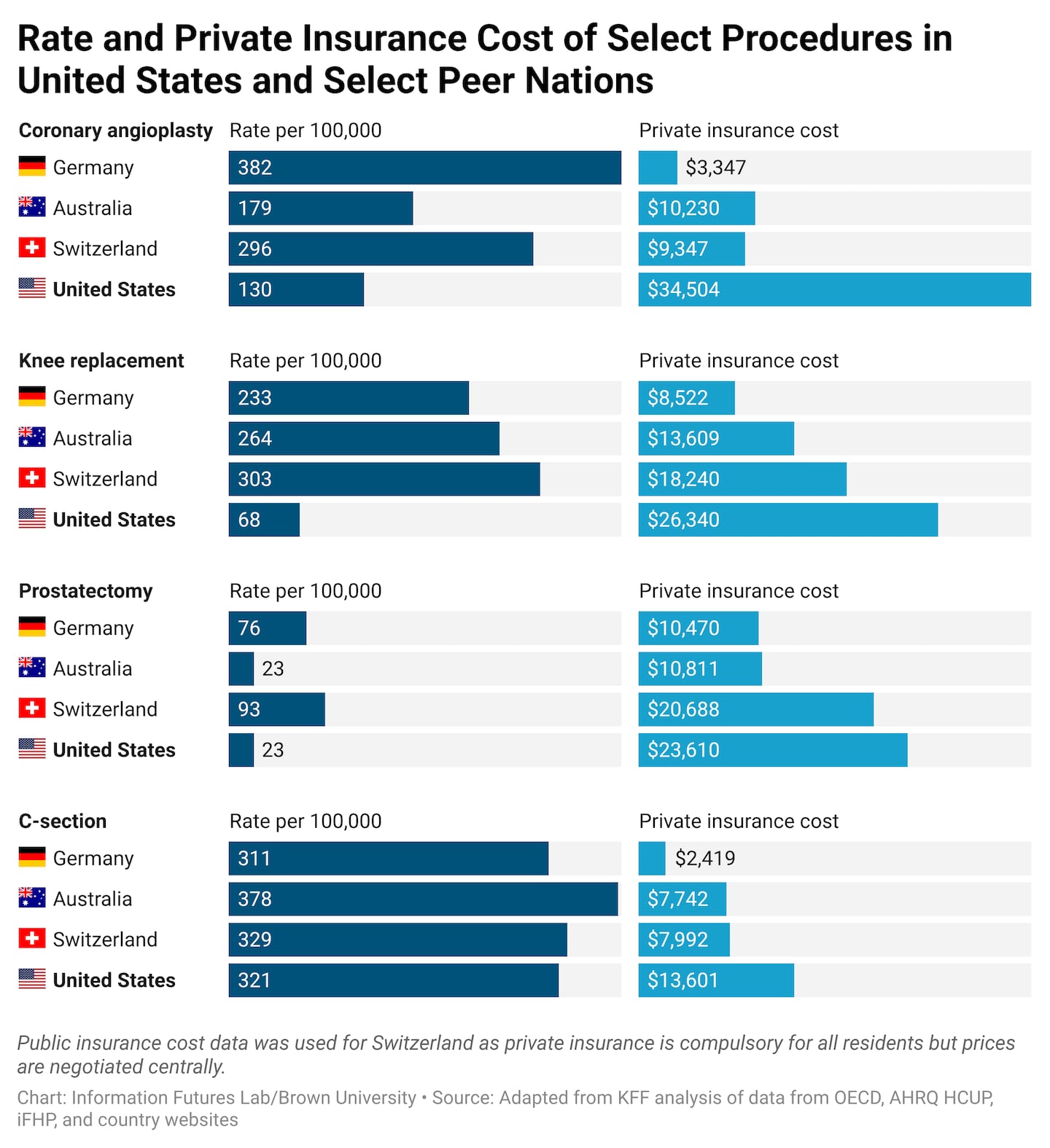
Americans don’t use health care more than people in other wealthy countries. But they pay more when they use it. These high prices show up in different ways, from higher premiums for consumers to slower wage growth when employers put more money into health care and less into salaries, to growing pressure on state budgets and small businesses.
 0309jhapricesInformation Futures Lab/Brown University
0309jhapricesInformation Futures Lab/Brown University
In most private contracts, prices are substantially higher than what Medicare pays providers. Health systems argue that they need these higher prices to compensate for underpayment from Medicaid or the uninsured. While there may be some truth to that argument, the real question is: How much is too much? In instances where markets are not functioning efficiently due to a lack of competition, what kind of prices should policy makers tolerate?
Recent analyses from RAND reveal that hospitals are paid, on average, roughly 2.5 times higher than what Medicare pays for the same services. But in some states, that average exceeds three times higher. And prices that are three times higher than Medicare rates are not rare; in parts of the country, they are the norm.
That reality suggests a straightforward, pragmatic reform. States could immediately cap commercial prices for all providers at 300 percent of Medicare, likely eliminating the most extreme excesses. The ceiling then could be gradually brought down over time (say, to 200 percent of Medicare over five years). Medicare rates were designed to sustain access and should be enough for a large number of providers to survive; twice that level should allow many well-run health systems to not merely survive, but thrive.
If this sounds radical, it really isn’t. In fact, the United States is the outlier when it comes to price regulation of private insurance markets. Most countries that rely on private insurance use price guardrails to make competition possible.
In Germany, multiple insurers compete, physicians operate independently, and patients have broad choice. But prices are shaped through negotiated national fee schedules. Hospitals are paid under structured frameworks rather than unconstrained local bargaining. Competition happens on quality and efficiency, and providers are prevented from exploiting market breakdowns to charge higher prices.
Switzerland, one of Europe’s most market-oriented systems, also relies heavily on private insurers and consumer choice. Yet prices are negotiated nationally with government intervention when negotiations fail. Not every service is priced the same way, but all operate within clear rules that limit how far prices can vary. Markets exist — but within boundaries. Other countries like the Netherlands also have private insurers operating under strong public oversight.
None of these systems is perfect. Each comes with trade-offs — controlling prices can mean less flexibility, more bureaucracy, or sometimes less innovation for truly groundbreaking treatments or services. But all begin from the same premise: Health care prices cannot be left entirely to local bargaining leverage in areas where there is inadequate competition to discipline prices. These international examples also underscore an important lesson: Regulating provider prices alone is not enough. In markets where insurers are concentrated, lower payments to providers won’t automatically translate into lower premiums for consumers because the dominant insurer can just pocket the savings. That is why many countries pair provider price limits with oversight of insurers, including insurance rate regulations.
Critics will argue that tying price caps to Medicare would destabilize health systems or threaten innovation. Those concerns deserve to be taken seriously. But a ceiling at 200 percent of Medicare prices still provides a generous margin above a payment system designed to ensure access nationwide.
Thousands of providers already deliver excellent care near those levels today. Some states are already moving in this direction, such as Vermont and Indiana, adopting price caps around this benchmark. More states, including Massachusetts, should do so to control costs. Failure to effectively run a financially sustainable system at twice Medicare rates suggests there are likely inefficiencies that can be rooted out.
Importantly, this approach would not require Washington to micromanage every medical service. States can adapt benchmarks to local conditions and phase them in gradually. The goal is not command-and-control pricing. It is establishing guardrails when markets fail to function effectively. When competition works, the government should step back. But when markets fail, refusing to act is a decision to let costs keep rising.
Markets need rules. And when markets fail to protect patients, policy should.