

Large-scale human data reveal that even a single antibiotic course may leave a measurable microbial footprint years later, raising important questions about long-term health effects and prescribing practices.

Study: Antibiotic use and gut microbiome composition links from individual-level prescription data of 14,979 individuals. Image Credit: marevgenna / Shutterstock
In a recent study published in the journal Nature Medicine, researchers found that antibiotic effects on the gut microbiome may persist far longer than expected. By linking Swedish prescription registry data with fecal metagenomic profiles from nearly 15,000 adults across multiple population-based cohorts, the study showed that even a single antibiotic course taken four to eight years earlier was associated with lasting differences in microbiome composition.
These findings highlight the potential for prolonged microbiome disruption and underscore the need for careful antibiotic use, as even routine prescriptions may have lasting health implications.
Gut Microbiome Disruption and Chronic Disease Risk
Disruptions to the gut microbial ecosystem are increasingly recognized as a key factor in a wide range of health conditions, including cardiometabolic disease, autoimmune disorders, and colorectal cancer. Antibiotics are a major driver of these imbalances, and repeated or prolonged use has been linked to higher risks of obesity, type 2 diabetes, and cardiovascular disease.
Small intervention studies have shown rapid declines in microbial diversity and shifts in key bacterial groups following treatment. However, these findings largely reflect short-term effects. As antibiotic use remains widespread, understanding long-term impacts on gut microbial communities has become a critical research priority, though robust large-scale evidence has been limited.
Population Study Design and Microbiome Analysis Methods
In this population-level study of 14,979 individuals, researchers examined the influence of oral antibiotic use over the previous eight years on gut microbial composition. They linked prescription data from the Swedish National Prescribed Drug Register (NPDR) with fecal metagenomic data from three cohorts: CArdioPulmonary bioImage Study (SCAPIS), Swedish Infrastructure for Medical Population-based Life-course and Environmental Research (SIMPLER), and Malmö Offspring Study (MOS).
The team assessed antibiotic exposure across three time windows: within 1 year, 1 to 4 years, and 4 to 8 years before sampling. Participants with recent antibiotic use, inflammatory bowel disease, or chronic pulmonary disease were excluded. Fecal samples underwent deep shotgun metagenomic sequencing, and microbial diversity was quantified using indices such as the Shannon Index and inverse Simpson Index. Taxonomic classification was performed using the Genome Taxonomy Database.
Multivariate regression models assessed associations between antibiotic exposure and microbiome diversity, adjusting for confounders including age, sex, body mass index (BMI), smoking status, education, and comorbidities. The models also accounted for medications such as proton-pump inhibitors (PPIs), statins, metformin, beta-blockers, antipsychotics, and selective serotonin reuptake inhibitors (SSRIs).
Sensitivity analyses tested alternative exclusion criteria, while spline-based models explored microbiome recovery over time. Subgroup analyses were conducted by age and sex.
Persistent Microbiome Changes After Antibiotic Exposure
Antibiotic use was common, with approximately 70–74% of participants having at least one prescription over the previous eight years. Broad-spectrum penicillins, penicillin V, and tetracyclines were most frequently used.
The largest reductions in microbial diversity occurred within 1 year of antibiotic use. However, significant associations persisted for exposures one to four years earlier and even four to eight years earlier. Each additional course was linked to further declines in diversity. Notably, even a single course taken years earlier was associated with long-term differences in the microbiome.
Clindamycin, fluoroquinolones, and flucloxacillin showed the strongest and most persistent effects. These antibiotics were associated with changes in the relative abundance of up to approximately 10–15% of microbial species. Beneficial species such as Alistipes communis and Odoribacter splanchnicus declined. In contrast, species associated with metabolic risk, including Ruminococcus gnavus, Flavonifractor plautii, and Eggerthella lenta, increased in abundance. Penicillin V showed relatively minimal effects.
Microbiome recovery was fastest within the first 2 years after antibiotic use but slowed thereafter and was often incomplete. Recovery varied by antibiotic class, sex, and age, suggesting that microbiome resilience differs across individuals. Sensitivity analyses confirmed the robustness of these findings.
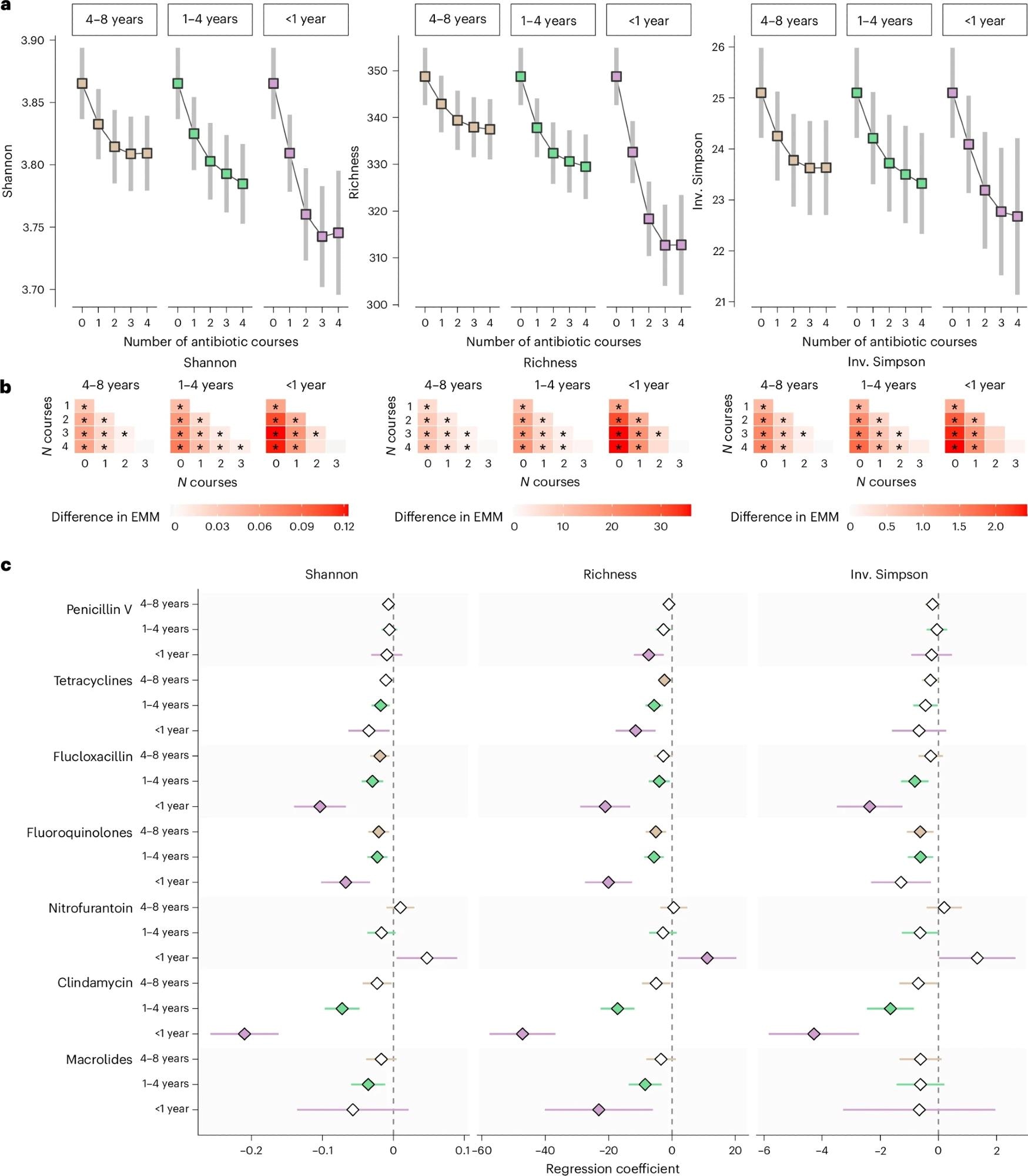
a, Microbiome diversity metrics (Shannon Index, species richness and inverse (Inv.) Simpson Index) for each additional course of any antibiotic 4–8 years, 1–4 years and <1 year before fecal sampling. Estimated marginal means (EMMs) of diversity were obtained using regression models, with antibiotic exposure modeled using restricted cubic splines and adjustment for age, sex, smoking, education, country of birth, site-specific analysis plate, BMI, Charlson Comorbidity Index, polypharmacy and use of PPIs, metformin, SSRIs, statins, beta-blockers and antipsychotics (n = 14,974). Squares represent the EMMs, and bars the 95% confidence intervals. b, Pairwise differences in EMMs of microbiome diversity by number of previous antibiotic courses. Stars indicate significant differences (FDR < 5%). c, Associations between antibiotic use in the 8 years before fecal sampling and gut microbiome species diversity were investigated using regression models adjusted for the same covariates as above, in three cohorts (SCAPIS, SIMPLER, MOS, total n = 14,974), followed by meta-analyses of the regression coefficients. The x axis and diamonds display the meta-analyzed regression coefficients; error bars represent 95% confidence intervals. Filled symbols indicate statistically significant associations (FDR < 5%). Antibiotics with at least one such association are shown.
Implications for Antibiotic Stewardship and Future Research
The findings suggest that some antibiotics may have long-lasting effects on the gut microbiome, persisting for more than four years. These results support more judicious antibiotic prescribing and stewardship strategies that minimize microbiome disruption.
However, the study remains observational and cannot establish causality. Further research is needed to understand long-term health consequences, including links to chronic disease. Findings may not generalize beyond outpatient settings in Sweden and may underestimate total antibiotic exposure due to missing hospital or international prescription data.
Journal reference:
Baldanzi, G. et al. (2026). Antibiotic use and gut microbiome composition links from individual-level prescription data of 14,979 individuals. Nature Medicine, 1-11. DOI: 10.1038/s41591-026-04284-y, https://www.nature.com/articles/s41591-026-04284-y